Nora Brown, MA, USAID; Sandra Dratler, DrPH, University of California, Berkeley; Muhammad Pate, MD, Duke University; Kristiana Raube, PhD, University of California, Berkeley; Will Mitchell, PhD, University of Toronto
Contact: William Mitchell, william.mitchell@Rotman.Utoronto.Ca
Abstract
What is the message?
This article describes the Mid-Level Management Training (MLMT) program in Nigeria, which provided ten months of health management training to about 100 clinical and administrative leaders in the Nigeria public primary healthcare sector from December 2009 through October 2010.
- The MLMT was organized by the National Primary Health Care Development Agency (NPHCDA) of Nigeria, with technical support from Duke University, the University of California at Berkeley, and the Global Business School Network in the U.S. Participants from 36 of Nigeria’s states and Federal Capital Territory undertook a series of six week-long residencies in Abuja, the capital of Nigeria.
- The summary evaluation of the program is that the curriculum identified relevant topics and that participants gained knowledge and confidence in the topics; moreover, the largest improvements occurred in a complex problem-solving exercise based on practical applications, which is arguably the most relevant evaluation.
What is the evidence?
Experience of the authors with the program, plus detailed program evaluations.
Links: Appendix A (curriculum philosophy) | Appendix B (curriculum detail)
Submitted: June 1, 2017; accepted after review, August 29, 2017.
Cite as: Nora Brown, Sandra Dratler, Muhammad Pate, Kristiana Raube, and Will Mitchell. 2017. Improving the Management Skills of Primary Healthcare Leaders: The “Mid-Level Management Training” Program in Nigeria. Health Management Policy and Innovation, Volume 2, Issue 2.
Introduction: The MLMT
In December 2009, eighty-four mid-level managers from primary healthcare facilities across Nigeria had thirty minutes to complete a problem-solving exercise:
“Assume that as a manager in a primary healthcare organization, you have been asked to come up with a plan to help your organization achieve an important element within one of the Millennium Development Goals by 2015. Using the data below, choose one area of focus for your plan:
[targets: (1) reduce child mortality; (2) reduce under-five mortality; (3) increase percentage of one-year-olds fully immunized; (4) reduce maternal mortality; (5) increase attended deliveries; (6) reverse the spread of HIV/AIDS; (7) reverse the spread of malaria]
In the next 30 minutes, outline a plan (using bullet points) using management approaches to achieve a MDG of your choosing. The management approaches may include skills such as statistics, computer applications, communication, strategy, financing, leadership techniques, client orientation, and monitoring & evaluation. Remember to focus on strategies that you as a manager can affect.”
Based on criteria from healthcare leaders and business faculty from the U.S. and Nigeria, the participants achieved a mean score of 32/100, ranging from 5 to 60. Clearly, there was room for improvement.
The test-takers were about to participate in the inaugural offering of the Mid-Level Management Training (MLMT) program, sponsored by the National Primary Health Care Development Agency (NPHCDA) of Nigeria. The MLMT would last until October 2010; the program included six week-long residencies held in the national capital, Abuja, plus inter-session projects.
The MLMT has a simple and powerful goal: To improve management skills so that public primary healthcare facilities can provide better services. With 170 million people, Nigeria is the most populous country in Africa. Health outcomes in the country are improving, particularly with increased emphasis on strengthening primary healthcare services; from 1990 to 2009–2010, life expectancy increased from 48 years to 54 years, while infant mortality during the first year of life decreased from 126 to 88 per 1,000 births.[1] Despite these gains, Nigeria has a long way to go to reach its Millennium Development Goals. The initial problem-solving exercise suggested that participants had opportunities improve their management skills and, in turn, help their facilities improve healthcare.
The World Bank’s 1999 report, Better Health for Africa (2), suggested that achieving better health is often constrained by poor management of health services. Limited but growing evidence from the gray literature of on-site reports and a small body of academic studies is beginning to document health management education programs (3–13). Reports suggest that most management education for health facility workers in low- and middle-income countries involves short courses. In parallel, there is growing interest in longer programs that are beginning to be developed at business and public health schools in Kenya, South Africa, Uganda, and elsewhere, sometimes with initial assistance from foreign universities. The MLMT program, sponsored by the NPHCDA, was designed to provide extended management education for middle-level managers in government-run healthcare facilities in Nigeria.
The NPHCDA is a parastatal agency linked to Nigeria’s Federal Ministry of Health, supporting more than 1,000 primary healthcare facilities (http://nphcda.org/index.php/history). The NPHCDA manages programs for vaccination, midwifery training, and other services (14). The agency views management training as a critical complement to its clinical services.
The MLMT was initiated by the CEO of the NPHCDA, Dr. Muhammad Pate (Dr. Pate later served as Minister for State for Health in Nigeria), together with agency staff members under the leadership of Dr. David Malgwi. Planning for the MLMT by staff members of the NPHCDA and faculty from a Duke University in the U.S., where Dr. Pate earned an MBA degree, began in 2009. The Health Sector Management program at Duke University’s Fuqua School of Business provided technical assistance for the inaugural MLMT.
Format and Participants
Curriculum
The MLMT teaches basic skills of general management and health policy, based on an approach of “contextualization in the classroom.” The format combines skills and experience of “content experts” who have knowledge of general management and health policy issues, together with “context experts” with relevant health sector experience.
The MLMT curriculum covered principles in twelve topics. The topics included epidemiology/statistics, leadership, financial management, communications, strategic planning, health economics, national healthcare policies, supply chain and logistics, quality of care, computer skills, and information systems. These topics encompass key elements of leadership and analysis.
Faculty from local institutions with experience teaching relevant concepts served as what the program referred to as content experts. These institutions included business and public health schools, plus Nigeria’s Center for Management Development. The faculty members were recruited via contacts of the NPHCDA.
Officials of the NPHCDA and several government agencies with relevant experience in practice served as what the program referred to as context experts. NPHCDA staff members have led vaccination, midwifery training, and other programs; this experience helped link management principles to participants’ experience. The NPHCDA also has extensive public- and private-sector contact, which helped identify other context experts.
The content and context experts worked together to plan and deliver sessions. Sessions, which usually lasted ninety minutes, typically included presentation of core principles by the content expert, examples of their use by the context expert, and ongoing discussion with the participants about their experience. Most sessions were followed by “skills stations” in which small groups of participants applied material from the sessions.
The six residencies, each lasting a week, contained subsets of the twelve core topics threaded together through the program. The threading reinforced topical interdependence. The appendices describe the program format in some detail.
Each participant applied the skills to an ongoing project at her or his facility between the sessions. Projects included improving data collection, expanding immunization and maternal and child health programs, conducting computer training in their organizations, and other topics. Participants provided updates and presentations about their work at the beginning of each session. Staff members from the NPHCDA reviewed the presentations and reports.
The program required substantial financial commitment. Core funding from the Head of the Civil Service of the Federation supported faculty stipends, program infrastructure (rental for training space and lodging, meals, and travel for participants), materials, and other expenses. The Bill and Melinda Gates Foundation supported international travel, materials development, and program evaluation. Duke’s Health Sector Management program supported initial travel costs.
Participants
Healthcare officials in each of Nigeria’s 36 states plus the FCT nominated five participants. The NPHCDA then invited three participants from each jurisdiction, basing choices on responsibilities, span of control, and education. Participants received invitations in early December for a program that would begin ten days later. Despite the short notice, 84 of the 121 invited participants joined the first session, with another 19 joining during the second session in February 2010 (people who joined in February came early for a two-day catch-up workshop). Of the 103 participants (55 men and 48 women), 96 remained through the final exam.
Participants had varied positions and responsibilities. The largest cohorts were healthcare administrators (32%), community health workers (27%), registered nurses (17%), and physicians (17%). Participants were responsible for community health education, maternal and child healthcare, immunization, communicable and non-communicable diseases, and other functions; more than half of the participants had at least two responsibilities (indeed, 17% reported responsibilities for “all PHC areas”). Most participants had substantial experience in their organizations (16.8 years mean) and current positions (5.0 years), with an average of 52 direct reports.
Evaluation: Relevance and Learning
The Global Business School Network (http://www.gbsnonline.org/) and two faculty members from the University of California Berkeley conducted five sets of within-subject evaluations.
Relevance and program evaluation
At the beginning of the program, participants indicated the frequency of use during the past three months (rarely, sometimes, often, always) of epidemiology, leadership, financial management, communications/presentations, and strategic planning. More than 50 percent of the individual participants used four of the five skills at least “often,” while epidemiology reached often-level use for just under 50 percent of individuals and more than 50 percent for their organizations. Hence, each area was relevant.
At the end of the program, the participants evaluated the quality of the MLMT. Scores reached 4.1/5 for instruction and assignments, 4.2 for participants, 4.4 for content, and 4.6 for relevance. Despite noting opportunities to improve, participants rated each aspect well.
Topical knowledge
Pre- and post-material evaluations focused on six subjects. The evaluation team used materials from the instructors and the team members’ knowledge of the topic to develop the tests. Each test included five to ten questions. Participants completed the post-assessments after the second session of each topic.
Scores improved in five topics (Table 1). Substantial gains occurred in epidemiology and health economics, which had the lowest bases (epidemiology: 48% to 65%; health economics: 51% to 60%). Strategic planning increased from 72% to 79%. The participants began with higher levels for leadership and communications, reflecting high use of these skills within their positions, yet still improved (leadership: 83% to 94%; communications: 81% to 88%). All five scores increased significantly (p<0.01, paired sample t-tests).
Table 1. Pre- and post-instruction tests of topical knowledge
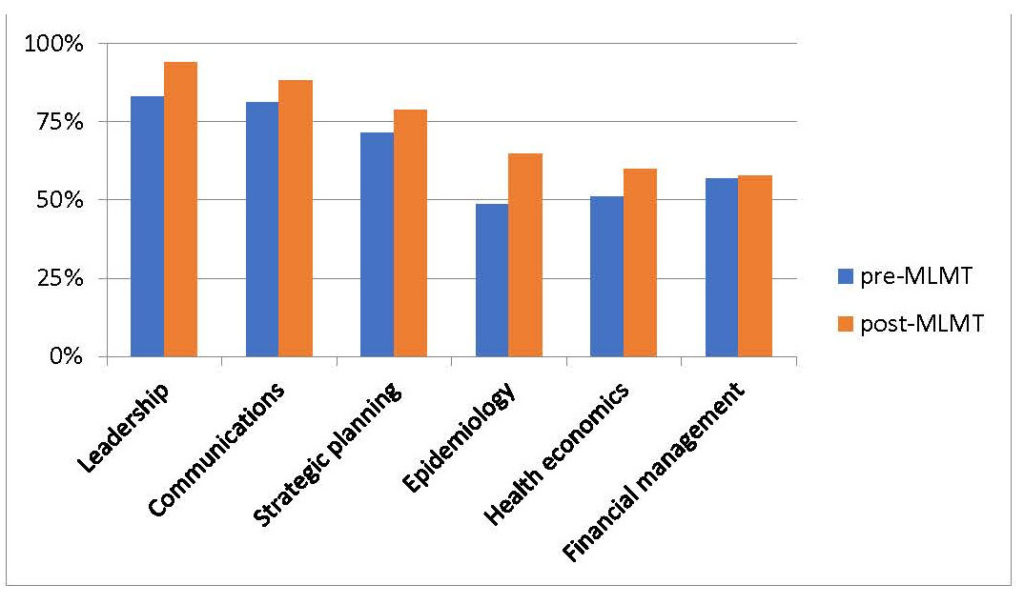
All five scores increased significantly (p<0.01, paired sample t-tests)
By contrast, financial management had little improvement after the second session (57% to 58%). The result for this topic may reflect initial choices of faculty, who had some difficulty connecting with the participants. After observing these results at a mid-point of the MLMT, the curriculum added a supplemental financial management class during the final session.
Confidence and empowerment
Before and after receiving instruction, participants reported their confidence in using six topics. Epidemiology, which had the lowest pre-instruction confidence, produced the greatest increase, from 3.4 to 4.3. For financial management, despite the relatively low test scores, confidence grew from 3.5 to 4.2. Participants indicated relatively high confidence initial levels in leadership, communications, and strategic planning; even these areas showed increased confidence by the end of the program (each moving from 3.9 to at least 4.1). Mean confidence in all six comparisons increased significantly (p<0.01; paired sample t-tests).
Pre- and post-program evaluations also found increased leadership empowerment, including making decisions and bringing about change. Average responses for empowerment to make decisions in participants’ current positions rose from 3.6 to 4.5; perceived ability to bring about change rose from 4.0 to 4.4 (both p<0.01; paired sample t-tests). Importantly, for both questions, the lower tails of the distributions rose substantially. More than a third of participants reported scores below 4 in the pre-program reports; fewer than 10 percent reported post-program scores of 3 (none below 3). The program appears to have helped participants who felt marginalized within their organizations gain self-assurance about their ability to lead.
Final exam
The participants completed a 100-question multiple-choice final exam, covering nine topics. Instructors provided the questions. The mean score was 76 percent (Table 2), ranging from 39 to 93 percent. Within topics, results ranged from 82 percent for individual leadership (9 questions) to 55 percent for communications (6 questions). The lower results for communications may arise because the instructors who set the questions were not those who delivered much of the material, so that the students may not have been tested on material that they learned.
Table 2. Final exam: Correct responses (96 participants)
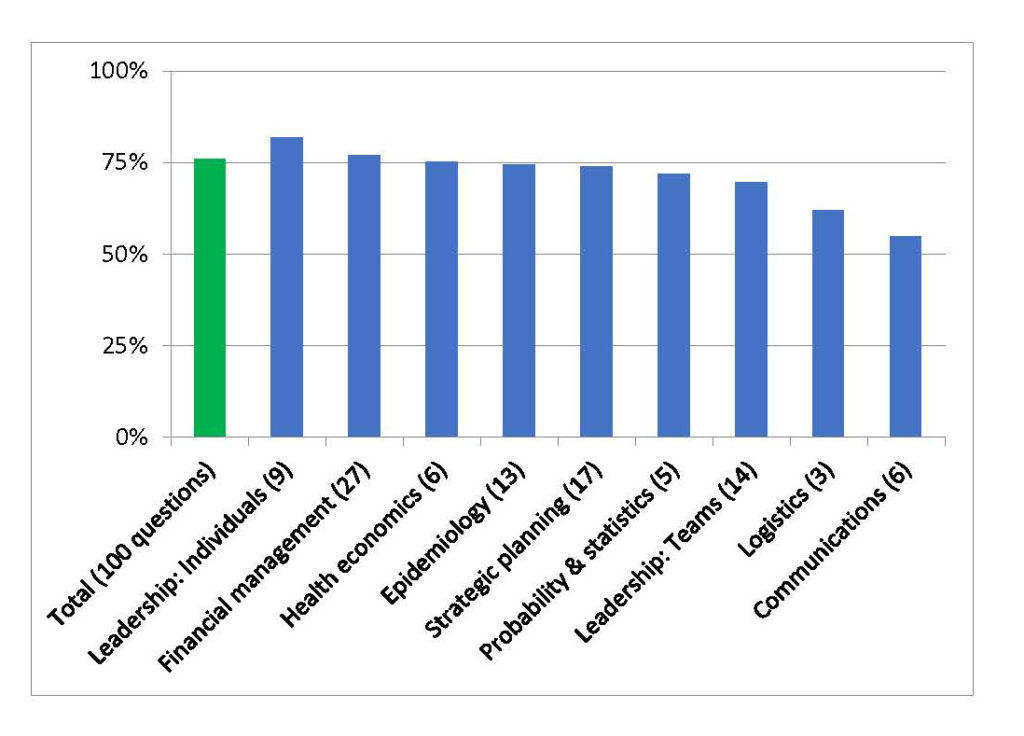
Intriguingly, the results for financial management (77%) were stronger than the results following the first two financial management sessions. The difference likely stems from the supplemental financial management session that occurred after the evaluations of the initial sessions reported limited learning.
Problem-solving exercise (PSE)
At the beginning and end of the MLMT, participants completed the problem-solving exercise we described in the introduction. The exercise sought to assess the integrative skills that they would need to address the complex problems that their organizations faced. The same team scored both PSEs. Scores rose substantially from December 2009 to October 2010 (Table 3): from means of 32 (range: 5 to 60) to 55 (range: 14 to 88) (p<0.01; paired sample t-test). Indeed, the final mean score approached the maximum initial score. This was strong evidence about the learning that took place during the course of the program.
Table 3. Pre- and post-program PSE results (77 participants)
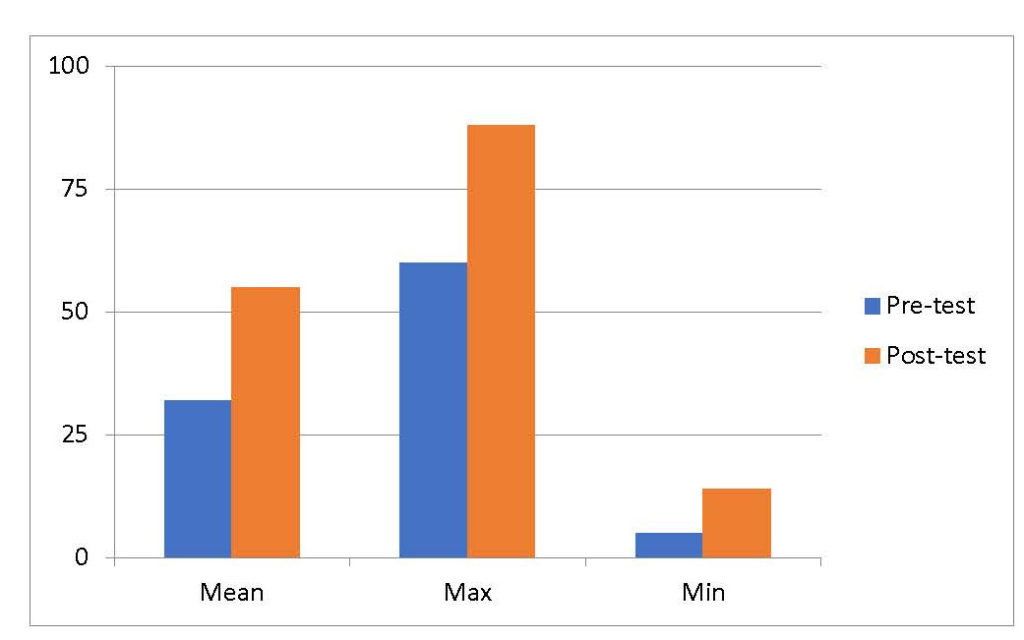
The pre- and post-program differences are statistically significant (p<0.01; paired sample t-test)
We investigated how the PSE scores related to education, sex, age, and years in organization or position. Only education level had a substantial relationship with PSE gains (r=0.36), and even there, the correlation arose from high starting scores and corresponding low increases for 11 participants at one of the lower levels of education (two-year national diplomas). Indeed, even three participants with the lowest education level (grade 12) moved from very low scores on the PSE pre-test to near the mean in the post-test. The main implication is that the program led to increased skills for participants with multiple backgrounds.
We also assessed correlations between PSE and final exam scores. Intriguingly, final exam scores had weak correlation with pre-program PSE (r=0.14) but stronger correlation with PSE increases (r=0.48) and post-program PSE (r=0.59). These results reinforce the conclusion that participants gained substantial knowledge.
Implications
The evaluations have two summary implications. First, the MLMT identified relevant topics. Second, participants gained knowledge and confidence in the topics. Moreover, the largest improvements occurred in the problem-solving exercise, which is arguably the most relevant evaluation—the complex challenges of the PSE reflect the practical activities that are the heart of the MLMT.
Clearly, the identification strategy of the evaluation has substantial limits. Although we examined multiple dimensions, the assessments investigated short-term impact and do not include a control group. We sought post-program review of the participants and their organizations, ideally including control groups who had not yet taken the MLMT, but logistic challenges made this impossible. The NPHCDA plans longer-term reviews as part of the ongoing MLMT.
We conclude by considering factors that underlay the initial successes of the MLMT and, in turn, opportunities that lie ahead. We stress that these points are not definitive conclusions, but rather offer a basis for discussion.
Success factors
We believe that the success of the MLMT stems from in achieving balance across what we refer to as the “tripod” of content, instruction, and program management.
Content is the first leg of the tripod. The emphasis on basic principles of core management, which the participants reported were highly relevant, coupled with active “contextualization in the classroom” was important. Contextualization connects the core skills to the participants’ daily management activities: in classroom sessions, skills stations, and ongoing projects. Contextualization helped provide robust frameworks with links to participants’ needs, plus relevant practice in using the frameworks.
Instruction is the second leg. Shared instruction by content and context experts linked framing with applications. The fact that local faculty provided almost all the instruction meant that lectures and discussion reflected the participants’ context. One of our favorite written evaluations from a session delivered by a non-local instructor (one of the authors) drove this point home for us: “What is this white guy doing trying to teach us? I don’t understand a word he is saying.” Even though all instructors, including local faculty, taught in English, effective communication required local nuance. Local faculty—whether academic instructors or practicing staff—could connect directly to the participants, speaking not just the formal language of English but also their daily language of practice.
Local program management is the third leg. Local staff organized the sessions, identified and communicated with participants and their superiors, and delivered the MLMT. Without local leadership, it would have been impossible to identify strong participants and, in turn, maintain their commitment through the ten months of the program. In parallel, local responsibility for primary funding created local commitment to the program.
Opportunities
Substantial work remains. First, discussion about content with participants suggests ongoing need to find a balance between generic management skills and relevant applications in the environments of Nigeria, a setting that is both heterogeneous across regions and dynamic across time. Moreover, there is a need for continued experimentation with combinations of in-depth instruction about topics within sessions and threaded instruction about related material across sessions.
Second, instruction generates multiple challenges. Participants evaluated most faculty members highly but did not connect well with a few instructors. Effective instruction requires faculty who are knowledgeable, engaged in the classroom, and willing to coordinate with other instructors. One of the takeaways from the initial differences in finance versus other topics was that success reflected instructors who worked closely with each other and engaged participants in discussions and applications.
In turn, at least four refinements have high potential. First, building a base of local materials would be valuable, particularly in translating generic skills into local contexts. Second, it would be useful to build “train the trainer” expertise for both classroom faculty and project mentors. Third, deeper collaboration with local business schools would help provide program management and instructional skills need for sustainability. Fourth, it would be useful to teach groups of colleagues from individual facilities, rather than bring only one individual at a time, or explicitly teach participants how to teach their colleagues back at home.
Clearly, management education needs to reach beyond the MLMT’s initial one hundred participants, to the thousands of people who provide primary healthcare services in Nigeria. We believe that the MLMT provides a strong basis for continuing health management education. The program contributed to the participants’ confidence and management knowledge. These skills are key complements to their clinical skills and the healthcare missions of their facilities.
Indeed, the MLMT has spawned a successor project. With initial support from the Nigerian Ministry of Health, the Gates Foundation, and local business leaders, in 2015, an independent Healthcare Leadership Academy (HLA) was established in the country.[2] Drawing on the lessons learned from the MLMT as well as other relevant programs, the HLA now offers regular health management programs for both public and private sector health care leaders in Nigeria. Thus, the initial success of the MLMT provided a stepping stone to a broader based initiative.
References
- World Health Organization. 2012. World Health Statistics, 2012. World Health Organization, Geneva.
- World Bank. 1999. Better Health in Africa: Experience and Lessons Learned. Washington, DC: The World Bank.
- Aina, O. 2011 (August 4). Health-care in Nigeria can’t improve beyond health workers capacity to manage WELL. Nigerian Health Journal. http://nigerianhealthjournal.com/?p=1219
- Briggs D.S., P. Tejativaddhana, M. Cruickshank, Fraser J, Campbell S. 2010. “The Thai-Australian Health Alliance: Developing Health Management Capacity and Sustainability of Primary Health Care Services”. Education for Health, 23 (3): 457.
- Egger D., P. Travis, D. Dovlo, L. Hawken. 2005. “Strengthening Management in Low Income Countries. Making Health systems Work”. Working Paper No.1, Department of Health Systems Policies and Operations. Evidence and Information for Policy. WHO/EIP/Health Systems. http://www.who.int/management/working_paper_1_en_opt.pdf.
- Egger D., E. Ollier. 2007. “Managing the Health Millennium Development Goals: The Challenge of Management Strengthening. Working Paper No. 8. Geneva: Department for Health Policy, Development and Services, Health Systems and Services, World Health Organization.
- Lee K., G. Walt, A. Haines. 2004. “The challenge to Improve Global Health: Financing the Millennium Development Goals. Journal of the American Medical Association, 291(21): 2636-8.
- Lewin S., J.N. Lavis, A.D. Oxman, G. Bastías, M. Chopra, A. Ciapponi, A. Flottorp, S.G. Martí, T. Pantoja, G. Rada, N. Souza, S. Treweek, C.S. Wiysonge, A. Haines. 2008. “Supporting the Delivery of Cost-effective Interventions in Primary Health-care Systems in Low-income and Middle-income Countries: An Overview of Systematic Reviews.” The Lancet, 372: 928-939.
- Management Sciences for Health. 2010. “Linking Management and Leadership Training to Service Delivery Outcomes”. Report on the impact of the Leadership Development Program (LDP) on service delivery outcomes in Kenya. http://www.msh.org/projects/lms/NewsRoom/upload/Kenya-LDP-4pager_2010-10-05.pdf.
- Mansour, M., J.B. Mansour, and A. HE Swesy. 2010. “Scaling Up Proven Public Health Interventions through a Locally Owned and Sustained Leadership Development Programme in Rural Upper Egypt.” Human Resources for Health 8:1. http://www.human-resources-health.com/content/8/1/1
- Moe J., C. Hope, L. Chhatwal, N. Homaifar, T. Koo, A. Maiga, G. Scheidler, M. Merson. 2008. “Private Health Sector Innovation in Response to the Human Resources for Health Global Crisis”, Report published by the Duke Global Health Institute. http://globalhealth.duke.edu/announcements/2008/DukeUniversityFinal_Report7-15-08.doc.pdf
- Thomas S., G. Mooney, S. Mbatsha. 2007. “The MESH approach: Strengthening Public Health Systems for the MDGs.” Health Policy, 83(2-3): 180-185.
- Travis, P., S. Bennett, A. Haines, T. Pang, Z. Bhutta, A. A. Hyder, N.R. Pielemeier, A. Mills, T. Evans. 2004. “Overcoming Health-systems Constraints to Achieve the Millennium Development Goals.” The Lancet, 364: 900-906.
- National Primary Health Care Development Agency of Nigeria. 2012. “2012 Nigeria Polio Eradication Emergency Plan” http://www.polioeradication.org/Portals/0/Document/Aboutus/Governance/IMB/6IMBMeeting/7.5_6IMB.pdf
[1] Rates for Africa in 2009–2010 were 54 years (life expectancy) and 75 deaths (infant mortality), compared to 76 years and 14 deaths in the Americas; 75 years and 11 deaths in Europe. (1)
[2] http://hlaafrica.org/