Stacy Wood, Poole College of Management and The Consumer Innovation Collaborative, North Carolina State University; Phoebe Crosthwaite, Stanford School of Medicine; Kevin Schulman, Stanford School of Medicine and The Graduate School of Business, Stanford University
Contact: kevin.schulman@stanford.edu
Abstract
What is the message? The explosion of interest around digital technology in healthcare has failed to spawn the requisite business model innovation. But advances in artificial intelligence and machine learning offer the opportunity for the deployment at scale of new care models based on largely unlimited supplies of intangible goods and services. Six types of subscription models in healthcare and non-healthcare markets can provide a novel pathway to support these evolving digital services, increasing patient access and engagement and price transparency.
What is the evidence? A comprehensive review of the different types of subscription models that can be applied to digital healthcare services.
Timeline: Submitted: January 31, 2025; accepted after review April 6, 2025.
Cite as: Stacy Wood, Phoebe Crosthwaite, Kevin Schulman. 2025. Not Just Netflix: Understanding Different Subscription Models and their Potential for Medicine. Health Management, Policy and Innovation (www.HMPI.org). Volume 10, Issue 1.
Key Words: Prevention, Primary Care, AI/ML, Financing Models
Background
The financing model for the U.S. healthcare system was largely codified with the establishment of the Medicare program in 1965. In it, health insurance would pay for services provided by physicians and hospitals, equating to the covered benefits of a contemporary Blue Cross/Blue Shield health insurance plan. Health insurance was not linked to services needed by beneficiaries, nor to health outcomes of individuals or populations. In many ways, by staying with this original design, health insurance models have become decoupled from (or even orthogonal to) our access to everyday healthcare services.
The discussion around AI in healthcare generally revolves around technology, and less frequently involves discussion of the business model needed to deploy the technology at scale. While many might consider a 60-year-old payment model to be ready for reassessment under any circumstances (the structure of how Medicare would pay for treatment was developed at roughly the same time that color television was first launched commercially in the United States), the emergence of digital healthcare services and artificial intelligence (AI) technologies make it urgent to reconsider this legacy model. At issue is how to organize the market and pay for the digital services that this technology can bring to patient care. This issue is made more challenging given that the use cases for AI are still evolving. To achieve cost and quality benefits from technology, we need technology innovation and business model innovation that develop in cooperation1 and that are not siloed from physician fee schedules2. Given the explosion of interest in digital technology in healthcare, what is remarkable is how little thought is going into business model innovation needed to deploy this technology.
One opportunity to consider as a novel market structure are subscription models. In general, subscription models involve a pre-payment to a subscription provider in exchange for easy access to a platform of goods and services for a set period. The subscription provider serves to organize the market for consumers. Borrowing from marketplace success in consumer goods, the idea of using subscription-style services in healthcare has recently been touted as a radical, but promising, route to improving healthcare access. Subscription-based healthcare includes formats like direct primary care (DPC), membership in fitness or health centers, and direct-to-consumer (DTC) platforms that offer set health services to members (e.g., Hims3). In contrast to capitation payment models which can restrict access to services, subscription models are designed to enhance ease of access to services for consumers by incentivizing providers to be proactive with regular care.
Research on healthcare subscription models has demonstrated promise in several populations, including patients with hepatitis C, obesity, cardiovascular disease, and those who are candidates for gene therapy (see Table 1 for a review of the current literature exploring subscription healthcare innovations). This idea is gaining increasing awareness; a recent industry study reported that 60% of surveyed employers were willing to contribute money to a monthly subscription care service and add it to their health plan4.
Table 1: Existing Literature on Subscription Models in Healthcare
| Author (year) | Premise |
| Glover et al., 202328 | Subscription model payment system for innovation in drugs (e.g. NHS subscription model pilot for antibiotics; fixed payments for antibiotic access)
|
| Trusheim et al., 201829 | The “Netflix model” for new treatments for HCV infections |
| Hampson et al., 202330 | Spreading payments over time. Increased certainty in the healthcare space as manufacturers receive fixed fee for supply and payers know what they are paying for/know for how long they will have access to that service. |
| Kirubakaran et al., 202331 | Subscription based model for remote health monitoring (mobile app/interface for a medical kit that allows for remote patient visits) |
| Dutta et al., 202032 | Subscription model/community financing for primary care in rural areas includes family-based membership, free consultations, medicine and lab discounts |
| Hohmeier et al., 202333 | Membership Pharmacy Model: partnership between pharmacy and employer, without the use of PBM (example: Good Shepherd Pharmacy (GSP) nonprofit community pharmacy – charges monthly membership fees, sells all prescriptions at acquisition cost) |
To date, advocates of subscription-styled innovations primarily urge the healthcare community to think of the operational model (and success) of Netflix5. Yet, by invoking Netflix in particular, discussions have been constrained to a limited view of subscription models which, unfortunately, undermines a full discussion of the value they can bring. In everyday life, subscription models go well beyond streaming services. Until we better understand the full range of different subscription types, we can’t assess their creative potential as a novel healthcare solution. While Netflix might be the best-known exemplar of the broader category, it may not be the type (or the only type) that best suits healthcare innovation. Thus, we describe an expanded framework of subscription models as they are commonly conceptualized in marketing research and offer examples of how they are currently used in- and outside of healthcare. What is clear from this review is that subscription models can provide workable models to increase access, engagement, and price transparency in medical care.
A Typology of Subscription Models
While the business world has made much of the recent boom in subscription models and its impact on consumers6, the concept is a long-established market model, and streaming platforms were not the pioneers in this space. Many of the earliest lending libraries in the 17th and 18th centuries were not public goods but were private subscription-based services and accessible only to members. Sepia images of paperboys and milkmen show the prevalence of 19th century subscription-based businesses. Many of us are familiar with common 20th century subscription models like gyms, public transport passes, and season tickets.
There are many different types of subscriptions, and, at a first pass, they can be divided into flat-fee and variable-fee formats. We define flat-fee subscriptions as those that offer either limited or unlimited services for a pre-determined and pre-paid cost per period. The individual may consume (or forego) the offerings available during the period. Variable-fee formats (or access-only subscription models) are essentially two-part tariffs, where payment confers access to services which are then consumed and paid for per use, often at a discounted price (e.g., an independent pharmacy that charges an annual membership fee and then sells drugs at their cost). In this review, we focus on flat-fee formats. Flat-fee formats, in general, increase price-transparency and reduce uncertainty because buyers can know and account for their future expenditures; preference for a flat-fee over variable-fees, even when the flat-fee is more expensive, is known as flat-fee bias7.
There are a surprising number of flat-fee subscription types (see Figure 1). Critically, they differ in a) the access model for goods and services (unlimited/limited), b) the primary benefit to the consumer/patient, c) the cost of the product/service, and d) the frequency of use of the product/service. Each category has some common consumer value (e.g., price transparency) that cascades to each category member. Additionally, each subscription type also has unique consumer value they offer.
Figure 1: Cascading Value in an Expanded Typology of Subscription Models
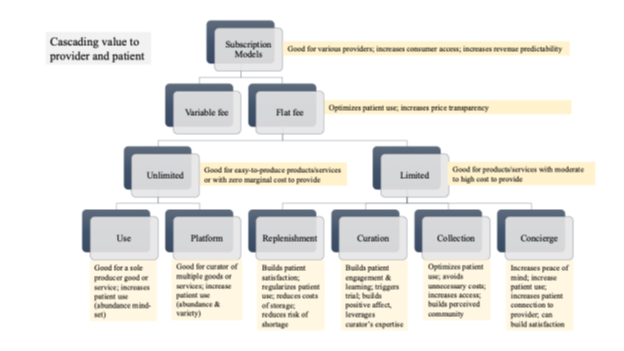
Figure 1 shows a framework of subscription model types and the common and unique value they provide to firms and consumers. Value descriptions are shown in yellow boxes; lower order branches have unique value and share the values of higher order branches.
For unlimited offerings, one can group subscription models into “unlimited use” and “unlimited platform” categories. Unlimited use refers to subscriptions where consumers receive unlimited “free” access for a set period to a product, service, or digital good (e.g., gym or museum membership, all-you-can-eat buffet, apps like Noom8 or Slack9). Here, the offerings are known beforehand and are stable; for example, the fitness machines at the gym generally don’t change. In these situations, the subscription provider has control or ownership of the offerings so that their availability and quality is reasonably static. Unlimited platforms offer the consumer unlimited access for a set period to a curated set of products, services, or digital goods on a common platform (Netflix, Hulu+10, the New York Times Digital Edition). In this case, the offerings are more dynamic, being either curated or obtained from other producers. The content may change noticeably from period to period. Unlimited Platforms like Netflix are undeniably attractive to consumers. Platforms also have tools to help patients identify the highest value content for their needs. These “recommender” algorithms could be based on patient input, physician input, or a combination of these two perspectives. In addition, “recommender” algorithms could promote novel content or services based on patient characteristics or diagnoses.
Research provides insight into how this model benefits consumers where the difference between consumer perceptions of “free” versus a small cost (such as the price of a movie ticket) can have significant effects on attitudes and behaviors11. Pre-payment for a period of unlimited usage creates a sunk cost against which consumers can view incremental usage as free and subsequently increase consumption12 .Additionally, the consumer benefits of unlimited supply are that they reduce planning-burden for those who are uncertain about their usage frequency13, stimulate consumption through a motivation to “get your money’s worth,”14 create a precommitment to usage of products and services that consumers believe they should consume (e.g., gym memberships), offer a perception of abundance that increases satisfaction15, and help build consumption habits through frequency of usage.
From a supplier perspective, unlimited use models are really scale models that spread the fixed cost of the platform (gym equipment, Netflix content, New York Times reporters) over a large subscriber base. They work best when the marginal cost of additional usage is relatively low cost (for example, the cost of serving an additional subscriber on the digital New York Times platform is essentially zero).
Limited use models are subscription models that offer a defined set of products and services on a periodic basis. These models differ from the platform models in that there is a non-zero cost to each marginal user (thus, the pricing model needs to account for the fixed costs of the platform and the cost of serving each user). Here, we describe four types of limited use subscription models: replenishment, curation, collection, and concierge subscriptions.
Replenishment subscriptions are those that provide consumers with regular delivery of the same high-frequency use products, services, or digital goods (e.g., Dollar Shave Club16, Amazon Subscribe & Save). Subscription providers may either produce the goods they deliver to consumers or may acquire them from manufacturers. The key consumer benefits that replenishment subscriptions provide are convenience, alleviating planning burden, and protection against shortages; the key supplier benefit is certainty in product demand and revenue. Consumers often over-estimate demand to avoid shortage17 but then also hold responsibility for the storage or discard of excess items. In some cases, having an excess of a product may independently trigger use (or even increased use) of the product18. Replenishment models may work for products/services at different price points and are best when consumption is both regular and frequent (for example, using this model for generic hypertensive medications).
Curation subscriptions offer consumers regular “gift-like” delivery of a novel or surprise set of products, services, or digital goods selected (often by experts) to match subscribers’ preferences (e.g., Birch Box19, Coffee of the Month, Stitch Fix20). In this way, curations allow consumers to explore product/service categories where they may be interested novices, enabling them to benefit from the expertise of others, and to interject self-care or “self-gifting” into their life21,22. Here, the novelty of what is received is important and so regular repetition (such as in replenishment) is negatively perceived. Because of the cultural norms of gifting, consumers may be inclined to perceive offerings more positively and to feel more satisfaction in what is received. Curations show a high degree of variability in the cost of products/services and in the frequency of their use. Successful curations fit consumers’ identity (i.e., “I am the sort of person who ___”) and may be time-limited as part of a larger goal (i.e., “This is my tool to learn about ___ or to get ___ under control”). For providers, offering different or rotating curations to consumer segments allows for smoothing demand (i.e., the firm does not have to provide 100% of consumers with the same “box” at the same time, but can design curations to fit supply patterns).
Collection subscriptions provide members with access to a shared set of products whose availability depends on other subscribers’ use (e.g., a public library, Community Toolshed programs, Rent the Runway23, Inspirato24). Thus, a community member may have easy access to some products but must wait for those in high demand. While libraries are a longstanding example, the academic business literature has been intrigued by the growth of these types of subscriptions because, for many product categories like clothing, they represent a dramatic shift from ownership to a sharing economy. Consumer interest in sharing a collection of expensive products like cars or very intimate products like clothes, rather than have the benefits and costs of ownership, has increased significantly. Here, individuals trade off access for cost-sharing, so these subscriptions are predominantly for high-cost, infrequent-use goods (e.g., ballgown, garden tiller, vacation home) where preferences may shift by occasion (e.g., a 4-wheel drive for a mountain trip and a sedan for a highway trip). Thus, collection subscriptions are very different from models that focus on relatively low-cost, frequent-usage goods like unlimited or replenishment models.
Concierge subscriptions offer consumers access to a shared set of services whose availability depends on other subscribers’ use; in this way, they are like a collection of (often human) service providers (e.g., Harper Concierge25, Duke Signature Care26). Subscribers benefit from committing a priori to the program for goods or services, such as a monthly carwash service for those who feel best in a clean car. They expect faster-than-normal access to services and may value this access as a status symbol, a time-saver, or both27. In practice, concierge medical subscriptions are often variable-fee models as they have a combination of unlimited and fee services; for example, medical concierge groups may offer unlimited calls, office visits, and simple tests, but charge separately for more complicated scans or treatments. In either case, the availability of the service provider is dependent on shared demand among subscribers, and so demand may outpace supply, especially at peak utilization seasons (flu season, for example). The success of concierge subscription models relies on access in practice and a balance of free and fee-based offerings. At this ideal position, the consumer feels that they are operating in a state of relative abundance, while the provider retains a profitable service model.
Figure 2: Descriptions and Examples of Flat-Fee Subscription Models
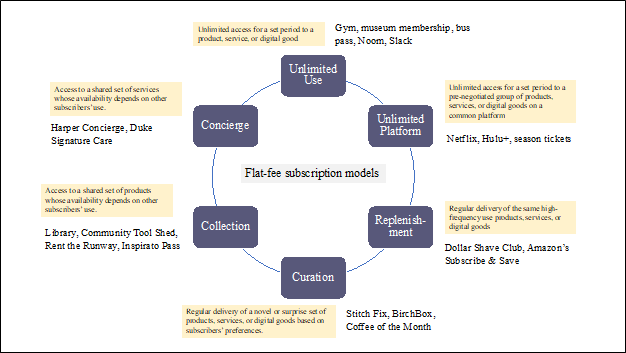
Figure 2 highlights the distinctions between different flat-fee models and emphasizes that providers can use one or a subset of these models (a “mix and match” strategy) based on the fit with care delivery in specific areas and the existing provider fee schedule.
Together, unlimited-use and limited-use subscription models have significant potential for healthcare adaptation, and several of these models are already deployed in the healthcare market today. They also offer significant opportunities for development of novel business models, especially when coupled with the emerging AI technologies. Table 2 outlines the six types of subscriptions we have described and how they could be used to build novel offerings in the healthcare market. Importantly, the diversity of subscription models prompts a more concrete and creative exploration of possible clinical uses based specifically on a) the type of service (e.g., human or digital), b) the benefit to the consumer (e.g., reduce planning burden or pre-commit to ideals), c) the benefit to the clinician (e.g., improved performance on population health metrics), and d) the potential for a sustainable business model. Payers that adopt subscription models can choose one, or a sub-set of subscription types in a “mix and match” strategy, based on unique patient populations or system goals.
Table 2: An Expanded View of Subscription Models and their Scope for Healthcare
| Subscription type | Benefit to patient | Current examples in healthcare | Potential healthcare use |
| Unlimited use | o Increase price transparency
o Reduce uncertainty in future expenses o Don’t need to predict usage frequency o Don’t need to conserve or skimp on usage o Increase consumption/usage to get money’s worth |
o Gym/fitness memberships
o Digital health apps, such as Headspace34 and Calm35 o Digital therapeutics, such as Big Health36 Akili37 o 24/7 clinical help lines o Some digital services in direct primary care (e.g. One Medical38, Parsley Health39, Curative40 |
o Smart device (Amazon Echo Show) with a therapy-specific skill to increase patient adherence
o Digital health coach to navigate services for key events (puberty, pregnancy, post-diagnosis, menopause) o Skin care AI app that allows patient to upload photos of moles. |
| Unlimited platform | o Increase price transparency
o Reduce uncertainty in future expenses o Don’t need to predict usage frequency o Don’t need to conserve or skimp on usage o Increase consumption/usage to get money’s worth o Dynamic or rotating products (novelty) o Wide array of products offered (variety-seeking) |
o Online platform that has access to variety of services (e.g. Hinge Health41)
o Online platform that has access to a variety of information and content (MyChart by Epic42]
|
o Smart device (Amazon Echo Show) with multiple therapy-specific skills for different outcomes
o Subscription to access a range of digital resources (sleep apps, mental health apps, nutrition apps) for general health or specific conditions o Platform with offering of various AI algorithms to serve patients holistically o Healthcare platform for patient visit coordination with prep and aftercare |
| Replenishment | o Convenience
o Efficiency (reduces planning/time burden) o Decreases risk of shortage o Regularizes consumption (prevents over- or underconsumption) o Avoids storage issues by minimizing surplus
|
o Online pharmacies that provide monthly access to/delivery of prescription medications (e.g. RxPass43 Nurx44) | o Monthly delivery of prescription medications/vitamins
o Program that delivers products covered by health insurance (sanitary products, sunscreen) o Regular delivery of treatments that have a regular but unusual schedule so that the patient uses/does the treatment as soon as they receive it (e.g., a patch that needs to be changed every 21 days) |
| Curation | o Novelty; element of ‘surprise’
o Discovery — provides patient with opportunity to try a range of products o Good for things where the patient wants to learn from an expert o Gifting or self-gifting framing creates more positive attitudes toward the sender and the things sent. o Builds trust and engagement when the curation fits the patient’s self-identity |
o Health/wellness boxes (e.g. Therabox45, Curology46) | o Monthly box with “freebies” that include tokens for medical services/products based on patient demographics
o Curations of digital app trials that spark interest in longer-term use (e.g., trial of Noom47, sleep apps). o Curations for patients with chronic conditions (for example, A1C level tests/CGM for people with diabetes. o Curations of screening tests or services to catch chronic disease early. o Curations to re-engage patients who have “fallen off the wagon” |
| Collection | o Price transparency
o Improves cost control o Decreased likelihood of skimping on needs or rationing of equipment o Don’t take on costs of ownership (repair, storage, discard) o Increases access to high-cost, infrequent-use goods |
o Medical Loan Closet of Henderson County48
o H.E.L.P (Health Equipment Loan Program) of Durham County49 o Concierge level rental program (e.g. Game Ready50) |
o Access to rent durable medical equipment for members/residents
o Short-term subscription to recovery equipment for specific procedure (e.g., ACL tear; Cardiac rehab) o Collection of athletic gear to encourage inactive patients to try different activities |
| Concierge | o Peace of mind
o Increased speed of access o A sense of status or prestige o Increased perceptions of personalized service o Convenience o Lowered planning burden o Self-identity as someone who prioritizes health |
o Direct Primary Care (DPC)
o Concierge medicine (e.g. Duke Signature Care51)
|
o Expanded use of DPC to provide specialty services for high-risk patients (e.g., COPD, skin cancer, mental health)
o Integration of human provider and digital services to increase coverage |
Application to AI
The revolution in AI is causing many sectors of the economy to pause and reconsider core business process and models. This pause asks the essential question of why we are doing what we are doing and might there be a better way to accomplish our goals. In this paper, we have identified a set of business models that can provide direct benefit to patients by providing a novel approach to service delivery for healthcare.
It is relatively easy to conceptualize unlimited platform subscription models as a means of organizing a set of digital services for patients. Platforms could acquire and curate algorithms to provide a complete set of offerings across populations. Platforms can be based in existing service delivery structures at the health system or payer level or could be based on new models of service delivery established in parallel with existing health insurance products or funded within or outside traditional health insurance plans. Platforms could also be coupled with other types of subscription models. Further, platforms could offer customized content views for different population groups stratified by age, race, gender, clinical condition, or language. This could provide a new pathway to help address health disparities by improving access to services and by building trust through new models of care.
What is also clear from this review is that the current payment models in healthcare are not designed to support value creation for consumers from direct applications of digital technology. For example, one can conceptualize a digital platform to support basic primary care and preventive services using a subscription framework (with access to technology and clinical services), but the current payment model supports only in-person physician visits (not even associated services like e-mail messaging).
Ultimately, the time is now for national healthcare stakeholders and established healthcare providers to think deeply about how we should organize the market for emerging services, especially digital services. Developing a novel market and allocating a dedicated stream of funding to that market is one means to spur development of technology that meets patients where they are throughout their care journey. Subscription models are a powerful means to consider as part of this discussion.
References
[1] Christensen CM, Bartman T, Van Bever, D. The Hard Truth About Business Model Innovation. MIT Sloan Management Rev. 2016; 58(1): 31-42.
[2] Berenson RA, Hayes KJ. The Road To Value Can’t Be Paved With A Broken Medicare Physician Fee Schedule. Health affairs. 2024;43(7):950-958. doi: 10.1377/hlthaff.2024.00299
[3] Hims & Hers Health, Inc. 2024. Accessed August 20, 2024. https://www.hims.com/
[4] Goforth A. Could subscription model be the answer to the US health care costs woes? Benefits PRO. June 27, 2022. Accessed August 20, 2024. https://www.benefitspro.com/2022/06/27/could-subscription-model-be-the-answer-to-us-health-care-cost-woes/?slreturn=2024071660621
[5] Netflix, Inc. 2024. Accessed August 20, 2024. https://www.netflix.com/
[6] Iyengar R, Park YH, Yu Q. The Impact of Subscription Programs on Customer Purchases. Journal of Marketing Research. 2022;59(6): 1101-1119. doi:10.1177/00222437221080163
[7] Nunes J. A Cognitive Model of People’s Usage Estimations. Journal of Marketing Research. 2000; 37 (4): 397-409
[8] Noom, Inc. 2024. Accessed August 20, 2024. https://www.noom.com/
[9] Slack technologies, LLC. 2024. Accessed August 20, 2024. https://slack.com/intl/en-ie/
[10] Hulu, LLC. 2024. Accessed August 20, 2024. https://www.hulu.com
[11] Shampanier K, Mazar N, Ariely D. Zero as a Special Price: the True Value of Free Products. Marketing Science. 2007; 26 (6): 742-757.
[12] Iyengar R, Park YH, Yu Q. The Impact of Subscription Programs on Customer Purchases. Journal of Marketing Research. 2022;59(6): 1101-1119. doi:10.1177/00222437221080163
[13] Nunes J. A Cognitive Model of People’s Usage Estimations. Journal of Marketing Research. 2000; 37 (4): 397-409
[14] Chandon P, Wansink B. Does food marketing need to make us fat? A review and solutions. Nutrition Reviews. 2012; 70 (10): 571-593. doi: 10.1111/j.1753-4887.2012.00518.x
[15] Lenglin V, Wong S, O’Callaghan C, et al. Evidence for involvement of the ventromedial prefrontal cortex is affective bias for free items. Cortex. 2023; 160: 24-42. doi: 10.1016/j.cortex.2022.12.009.
[16] Dollar Shave Club. 2024. Accessed August 20, 2024. https://us.dollarshaveclub.com/
[17] Nunes J. A Cognitive Model of People’s Usage Estimations. Journal of Marketing Research. 2000; 37 (4): 397-409
[18] Chandon P, Wansink B. Does food marketing need to make us fat? A review and solutions. Nutrition Reviews. 2012; 70 (10): 571-593. doi: 10.1111/j.1753-4887.2012.00518.x
[19] Birch Box. 2024. Accessed August 20, 2024. https://www.birchbox.com/
[20] Stitch Fix. 2024. Accessed August 20, 2024. https://www.stitchfix.com/
[21] Mick D, DeMoss M. Self-Gifts: Phenomenological Insights from Four Contexts. Journal of Consumer Research. 1990; 17 (3): 322-332.
[22] Kivetz R, Simonson I. Self-control for the Righteous: Toward a Theory of Precommitment to Indulgence. Journal of Consumer Research. 2002; 29(2): 199-217. doi: 10.1086/341571
[23] Rent the Runway. 2024. Accessed August 20, 2024. https://www.renttherunway.com/
[24] Inspirato. 2024. Accessed August 20, 2024. https://www.inspirato.com/
[25] Harper. 2024. Accessed August 20, 2024. https://www.harperconcierge.com/
[26] Duke University Health System. 2024. Accessed August 20, 2024. https://www.dukehealth.org/treatments/duke-signature-care
[27] Belleza S, Paharia N, Keinan A. Conspicuous Consumption of Time: When Busyness and lack of Leisure Time Become a Status Symbol. Journal of Consumer Research. 2016; 44(1): 118-138. doi: 10.1093/jcr/ucw076
[28] Glover R, Singer A, Roberts A, Kirchhelle C. Why is the UK subscription model for antibiotics considered successful? The Lancet Microbe. 2023; 4(11): E852-E853. doi: 10.1016/S2666-5247(23)00250-1
[29] Trusheim M, Cassidy W, Bach P. Alternative State-Level Financing for Hepatitis C Treatment – The “Netflix Model” JAMA. 2018; 320 (19): 1977. https://doi.org/10.1001/jama.2018.15782
[30] Hampson G, Steuter L. Netflix and pill: is there a role for volume-delinked subscription-style payments beyond antimicrobials? Expert Review of Pharmacoeconomics & Outcomes Research. 2024; 24 (1): 1-3. doi: 10.1080/14737167.2023.2271171
[31] Kirubakaran S, Gunasekaran A, Dolly R, Jagannath D, Peter D. A feasible approach to smart remote health monitoring: Subscription-based model. Frontiers in Public Health. 2023; 11. doi: 10.3389/fpubh.2023.1150455
[32] Dutta M, Mohan P, Mohan S, Ponnappan V, Satyavageeswaran P. Financing primary healthcare for rural areas. Journal of Family Medicine and Primary Care. 2020; 9(11): 5516-5522. doi: 10.4103/jfmpc.jfmpc_1131_20
[33] Hohmeier K, Baker P, Storey C, Martin N, Gatwood J. Exploring the Membership Pharmacy Model: Initial impact and feasibility. Journal of Pharmacists Association. 2023; 63(2): 672-680. doi: 10.1016/j.japh.2022.10.014
[34] Headspace, Inc. 2024. Accessed August 20, 2024. https://www.headspace.com/
[35] Calm. 2024. Accessed August 20, 2024. https://www.calm.com/
[36] BigHealth. 2024. Accessed August 20, 2024. https://www.bighealth.com/
[37] Akili, Inc. 2024. Accessed August 20, 2024. https://www.akiliinteractive.com/
[38] 1Life Healthcare, Inc. 2024. Accessed August 20, 2024. https://www.onemedical.com/
[39] Parsley Health. 2024. Accessed August 20, 2024. https://www.parsleyhealth.com/
[40] Curative, Inc. 2024. Accessed August 20, 2024. https://curative.com/
[41] Hinge Health, Inc. 2024. Accessed August 20, 2024. https://www.hingehealth.com/
[42] Epic Systems Corporation. 2024. Accessed August 20, 2024. https://www.epic.com/about/
[43] Amazon.com, Inc. 2024. Accessed August 20, 2024. https://pharmacy.amazon.com/rxpass
[44] NURX, Inc. 2024. Accessed August 20, 2024. https://www.nurx.com/
[45] Therabox.2024. Accessed August 20, 2024. https://mytherabox.com/
[46] Curology. 2024. Accessed August 20, 2024. https://curology.com/
[47] Noom, Inc. 2024. Accessed August 20, 2024. https://www.noom.com/
[48] Emerge Multimedia, LLC. 2023. Accessed August 20, 2024. https://medicalloancloset.org/
[49] Project Access of Durham County. 2024. Accessed August 20, 2024. https://projectaccessdurham.org/projects/health-equipment-loan-program/
[50] Avanos Medical, Inc. 2024. Accessed August 20, 2024. https://gameready.com/
[51] Duke University Health System. 2024. Accessed August 20, 2024. https://www.dukehealth.org/treatments/duke-signature-care