David Scheinker, Andrew Shin, and Rick Majzun, Lucile Packard Children’s Hospital, Stanford University
Contact: dscheink@stanford.edu
Abstract
What is the message? This is the first major study into how hospitals can improve operational efficiency by adopting aviation’s integrated approach to operational improvement since the U.S. Institute of Medicine reported 25 years ago that hospitals could reduce errors and patient harm by adopting aviation’s systems-based approach to safety. The authors demonstrate that from 1995 to 2019, aviation labor productivity increased by 247% and the price of an average roundtrip declined by 28%, while hospital labor productivity declined by 1% and per-capita national expenditures increased by 287%. Using counterfactual analysis, they estimate that if hospitals expenditures fell at half the rate of airline prices over the period studied, cumulative national hospital expenditures would have been $9.22 trillion lower ($18.24 trillion actual vs. $9.02 trillion counterfactual), with annual savings increasing from $21 billion in 1996, 0.25% of GDP, to $838 billion, 3.9% of GDP, in 2019.
What is the evidence? The comparison of cumulative growth in labor productivity, prices, and expenditures for hospital care and aviation from 1995 to 2019 using data from the Bureau of Labor Statistics, Bureau of Transportation Statistics, and the Centers for Medicare and Medicaid National Health Expenditures. The authors examined the average price of domestic roundtrip airfares and the national per-capita expenditure on hospital care, both measured in inflation-adjusted 2025 dollars, and illustrate differences between how hospitals and airlines improve productivity, manual versus digital scheduling, and sequential versus integrated optimization.
Timeline: Submitted November 21, 2025; accepted after review January 14, 2026.
Cite as: David Scheinker, Andrew Shin, and Rick Majzun, Stanford University. 2026. Inefficiency is Human: Engineering a More Productive Hospital System. Health Management, Policy and Innovation (www.HMPI.org). Volume 11, Issue 1.
Introduction
The United States healthcare system faces a persistent cost crisis. National health expenditures reached $4.9 trillion, representing 17.6% of GDP, with hospital care alone accounting for $1.5 trillion.[1] Over the past three decades, national expenditures on hospital care have increased at rates consistently exceeding GDP growth, straining households, businesses, and government budgets. Out-of-pocket expenditures alone totaled $506 billion in 2023. Spending growth is commonly attributed to factors inherent to healthcare: expensive new technologies, an aging population with a high burden of chronic disease, and high prices negotiated between hospitals and insurance companies.
The U.S. aviation industry—another complex, highly regulated sector—tells a strikingly different story. Despite facing similarly stringent regulatory oversight from the Federal Aviation Administration (FAA), complex operational challenges, unionized workforces, and substantial capital requirements, airlines have achieved dramatic productivity gains. Real air travel costs, measured as average domestic roundtrip fares in inflation-adjusted dollars, have declined steadily over the past 30 years despite rising fuel costs.
The similarities between aviation and hospital care were first highlighted in the Institute of Medicine’s seminal report, To Err is Human. [2] That work exposed the unacceptably high rates of patient harm and death associated with healthcare errors and described how focusing on system-level improvements — rather than individual performance — could reduce them. The report underscored structural, operational, and regulatory similarities between aviation and healthcare, including high capital costs, extensive regulations, and large, interdependent workforces. It identified how airlines engineer safety into their processes, rather than rely on individual vigilance, and enumerated opportunities for hospitals to design similar system-based approaches to safety and quality.
To Err is Human made a compelling case that lessons from aviation are valuable for hospital leaders despite the profound differences between the industries. This work examines the divergent trajectories of labor productivity and national spending in U.S. hospitals and airlines. We identify the system-level strategies that have enabled airlines to sustain productivity growth and explore how similar principles could be adapted to improve efficiency, safety, and outcomes in hospitals and other healthcare systems.
Background
Industry Similarities and Differences
Hospitals and airlines share several key characteristics that make for appropriate comparisons of their productivity.
Regulatory
Hospitals and airlines operate under extensive regulatory oversight: hospitals by the Centers for Medicare & Medicaid Services (CMS), the Food and Drug Administration (FDA), and state agencies; and airlines by the FAA and Department of Transportation (DOT). In addition to setting numerous licensing, reporting, and administrative requirements, the regulators restrict capacity by, for example, limiting the number of licensed beds a hospital may operate and tightly controlling airspace where aircraft may fly.
Capital, Workforce, and Safety
Both industries demand substantial capital investments in infrastructure and equipment, rely on highly skilled unionized workforces, and operate continuously with complex demands to schedule and coordinate service. Each faces rigorous safety requirements, where failures carry severe consequences, and handles sensitive data that must be protected. Ultimately, both must balance operational efficiency with service quality in high-stakes environments where errors can be catastrophic. [2]
Contractual
In both industries, incentives are constrained by contractual relationships with non-customer counterparties. Hospitals negotiate with, and are primarily reimbursed by, public and private insurance companies. Airlines negotiate with, and pay landing fees, gate rental charges, and other usage fees, to publicly-owned airports.
Competitive environments
The arguments for why lessons from airlines are valuable for hospitals, despite their differences, are beyond the scope of this work. However, differences in their competitive environments warrant attention. The airline industry has a high level of price competition with extremely price-sensitive consumers and highly sophisticated pricing algorithms. In contrast, hospital payments are dominated by private and public third-party payers who negotiate long-term contracts at fixed prices, leading to relatively little consumer price-sensitivity and thus, price competition (in fact, prices are usually opaque to consumers and care providers). Weaker price competition weakens hospital incentives to reduce prices. However, hospitals still have strong incentives to increase profits by improving labor productivity and efficiency in order to reduce costs. [3]
Labor Productivity in Aviation
Algorithmic Contracting
Airlines negotiate multi-year use and lease agreements with airports that formalize incentives for airlines and airports to be efficient. These contracts use sophisticated rate-setting methodologies to encourage airlines and airports to bear financial risk for their volume of service and the efficiency of their operations, and are shaped by quantitative analyses of non-aeronautical revenue (shops, restaurants, parking lots and hotels) and aeronautical revenues (passenger and airline fees). [4,5] For airports, service-level agreements specify performance targets for turnaround times, facility availability, and passenger throughput, with penalties for underperformance and bonuses for exceeding benchmarks. Empirical data suggest that contract design effectively shapes organizational incentives, finding that well-designed contracts yield 18% to 23% higher operational efficiency than contracts where airlines guarantee airport revenues regardless of performance. [6]
Digital Scheduling
Airlines’ transition to self-service digital sales channels eliminated approximately $3 billion in annual costs associated with travel agent booking fees and call center labor expenses.[7] This shift improves customer convenience and allows airlines to implement real-time revenue management algorithms that adjust prices based on demand patterns and seat availability to maximize revenues and fleet efficiency. Algorithmic pricing systems, pioneered by airlines in the 1980s, generate revenue increases and improve the availability of desirable seats by, for example, offering price-sensitive travelers advance-purchase discounts and offering time-constrained travelers booking on short increased availability at higher prices. [8]
Integrated Mathematical Optimization
The airline industry has been a leading adopter of operations research and optimization techniques since the 1960s. [9-11] A well-known 1969 survey of crew scheduling optimization — one of the top cost drivers for airlines — detailed how airlines use various mathematical techniques to minimize crew scheduling costs while meeting safety regulations, union requirements, and company policies. [9] The following half century has seen steady progress in the use of optimization to schedule larger crews more efficiently. In 1991, American Airlines reported that their TRIP system saved $20 million annually through optimized crew pairing [12]. Today, sophisticated software solutions from vendors like Jeppesen (Boeing), Sabre, and IBS Software achieve, 3% to 15% reductions in crew-related costs through modern mathematical programming approaches [13]. More broadly, airlines use mathematical optimization to improve many aspects of their operations, from flight scheduling to aircraft routing, transforming operational efficiency across the industry. [14]
Labor Productivity in Healthcare
Ad-hoc Contracting
Most hospitals negotiate hundreds of separate payer contracts with varying reimbursement methodologies, quality metrics, and reporting requirements that create administrative burden without systematic incentives for operational efficiency. A significant fraction of hospital revenue comes from fee-for-service contracts negotiated as a fraction of hospital charge master list prices, meaning that providing more care leads to higher payments while improved efficiency can reduce reimbursements. [15] Even the move toward value-based contracting, intended to create incentives for more efficient care, has led to more changes in how patient care is coded than to improvements in how care is delivered.
Manual Scheduling
Most hospitals continue to operate labor-intensive scheduling call centers that preclude: algorithmic optimization of appointment scheduling, self-service patient portals, and dynamic pricing mechanisms to balance demand across time slots or incentivize patients to choose underutilized appointment times.[16]
Sequential Manual Optimization
Hospital and health system operations present numerous opportunities to improve efficiency through optimization technologies: scheduling patient hospital admissions or clinic visits; scheduling nurses to units or shifts; allocating operating room time and block schedules; sequencing elective and urgent surgical cases; and assigning hospital services to specific units. [16-19] Although these aspects of operations drive significant costs and revenues, hospitals have been slow to adopt optimization-based approaches to improve operational efficiency. Electronic Health Record (EHR) systems, now nearly universal, are primarily designed to support clinical documentation, billing, and regulatory compliance than to optimize operational efficiency [20]. A vast literature documents the unrealized potential of EHRs to improve quality and efficiency. [21,22]
Data and Methods
Productivity and Cost Data
Measuring productivity in service industries poses well-documented challenges. The Bureau of Labor Statistics (BLS) defines labor productivity as output per hour worked, but defining “output” for hospitals and airlines requires careful consideration described in industry-specific publications.[23,24] For hospitals, BLS developed a new methodology in 2015 based on counting courses of treatment (inpatient stays and outpatient visits) classified by diagnostic type, representing a substantial improvement over earlier deflated-revenue approaches.[23] For aviation, BLS measures labor productivity as an index of gross output, which is based in large part on passenger miles divided by the labor input index. [24]
Hospital labor and aviation labor productivity data were extracted from the BLS Industry Productivity Studies program. [25] Hospital expenditure data and the population used to calculate per-capita expenditures were extracted from the CMS National Health Expenditure data. [1] Average annual airfare cost data were extracted from the Bureau of Transportation Statistics.[26]
Counterfactual analysis
To estimate the potential savings associated with labor productivity improvements, we calculated the reduction in annual hospital expenditures each year from 1996 to 2019 as follows. From 1995 to 1996, per-capita hospital expenditures increased by 2.2% while average aviation prices declined by 7.8%. We estimated the counterfactual 1996 hospital per-capita spending by reducing the 1995 per-capita spending by half the corresponding reduction in aviation (3.9%) and extrapolating to the entire population to account for population growth. For 1997, we used the adjusted counterfactual 1996 per-capita expenditures as the baseline and adjusted it by half the 1996 to 1997 cost reduction in aviation. We repeated this for subsequent years.
Results
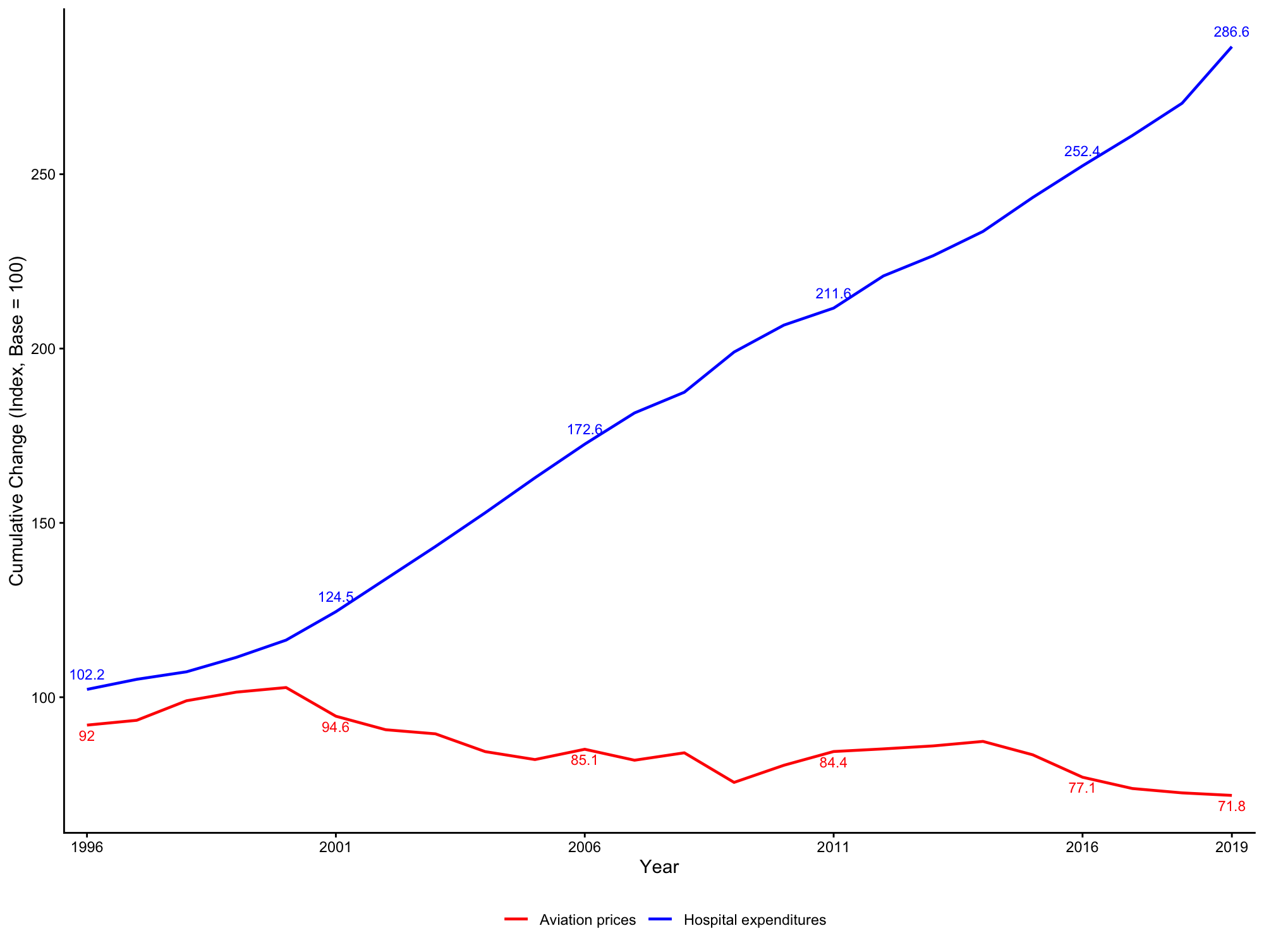
From 1995 to 2019, aviation labor productivity increased by 247% and the average price of a round trip declined by 28%, while hospital labor productivity declined by 1% and per-capita expenditures increased by 287% (Figure 1, Figure 2).
Figure 1: Aviation and hospital cumulative annual labor productivity growth
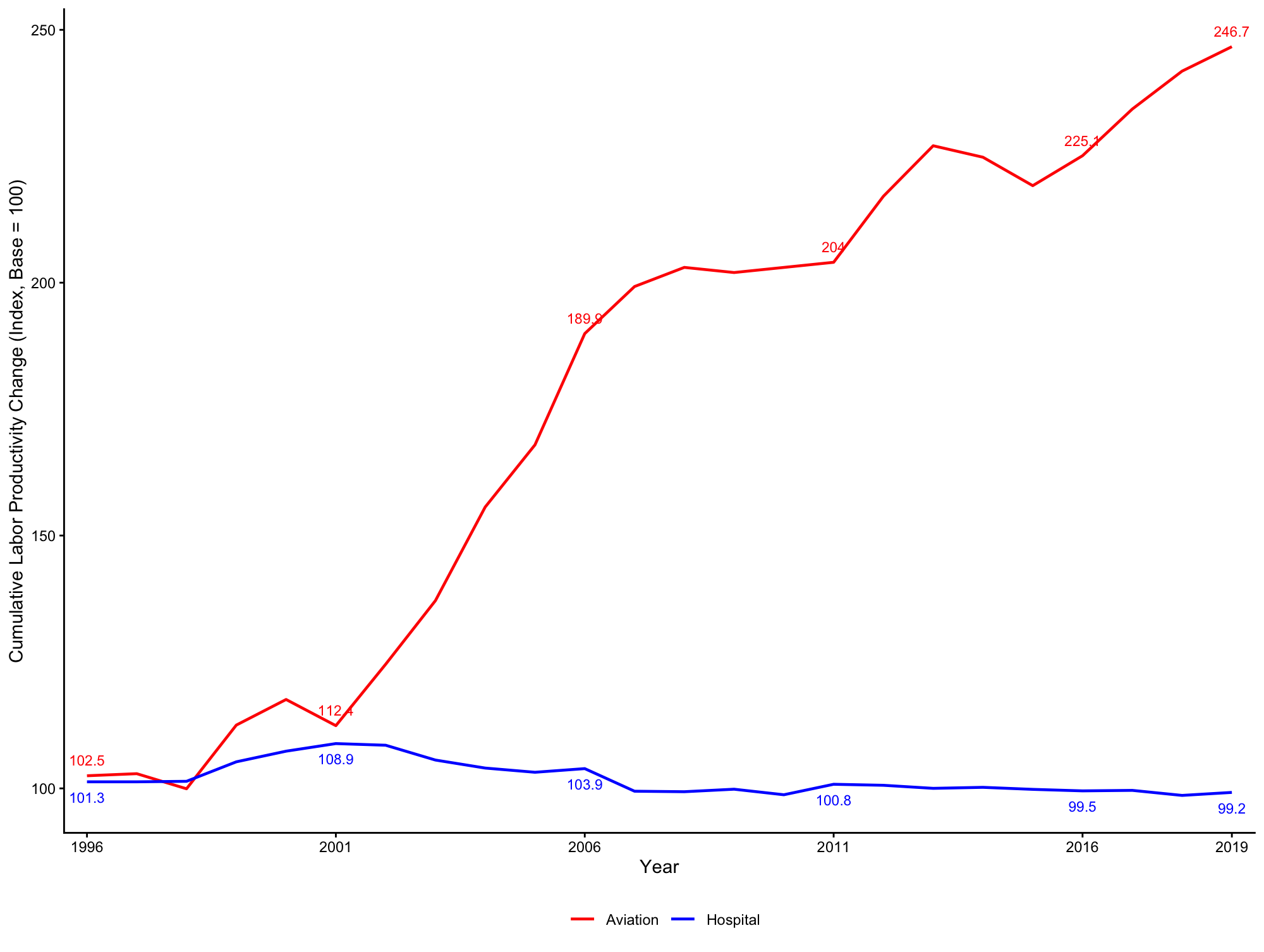
Figure 2: Aviation price and hospital per-capital expenditure cumulative annual growth
Counterfactual analysis
From 1995 to 2019, total hospital expenditures in 2023 dollar amounts were $18.24 trillion. A reduction in hospital expenditures corresponding to 50% of the corresponding annual price reduction in aviation costs, corresponds to $9.02 trillion, a savings of $9.22 trillion. From 1996 to 2019, hospital expenditures and cumulative savings in aviation increased, from a baseline expenditure of $350 billion in 1996, with a potential savings of $21 billion, to an expenditure of $1,193 billion in 2019, with a potential savings of $838 billion.
Discussion
In our analysis of 25 years of labor productivity, price, and expenditure data for U.S. aviation and hospital care, we found that the aviation industry achieved significant productivity gains and price reductions, while hospital labor productivity remained essentially unchanged and expenditures rose by nearly 300%. Our counterfactual analysis suggests that improving hospital labor productivity at a fraction of the rate achieved in aviation, would correspond to a reduction of expenditures by hundreds of billions of dollars, assuming those savings are passed on to consumers. These findings, along with the success of the safety practices hospitals adopted from airlines, suggest that hospitals should further investigate airline labor productivity practices.
Although limited rigorous research is available, available data suggest that hospitals spend far less on technology that improves productivity than do airlines. Interviews with the Chief Informatics Officers (CIOs) of nine hospital systems found that over 70% of the information technology budget is typically spent on maintenance versus 10% to 20% for innovation. One CIO reported that he, “spends 70% of his time thinking about transformation and 70% of his team’s resources on maintenance.” [27]
Our quantitative findings align with limited data contrasting how hospitals and airlines allocate spending on consulting services. McKinsey & Company, one of the largest healthcare consultants employing 1,700 healthcare-focused advisors, reported $20 million in earnings in a single year from one hospital chain. [28] Their focus, and the more general focus of healthcare consulting, tends to center on strategic planning, mergers and acquisitions, and regulatory compliance rather than mathematical optimization of operational efficiency.
In contrast, Boston Consulting Group, another large consultancy, reports helping one large U.S. airline reduce operational costs by 20% to 25% by optimizing crew staffing, improved maintenance scheduling, and higher airport utilization. This work, along with other consulting work in aviation, emphasizes the deployment of mathematical models to facilitate operational efficiency gains. Even more broadly, the use of cutting edge mathematical modeling is so established in aviation that students commonly pursue graduate degrees in operations research of industrial engineering with the intent of subsequently working in aviation.
This divergence in consulting focus likely both reflects and perpetuates the productivity gap between hospitals and airlines. Hospitals purchase consulting services for strategy and compliance; airlines purchase them for operational optimization. The consulting industry responds to client demand, creating a self-reinforcing cycle where hospitals receive relatively little consulting support for the operational improvements that drive airline productivity.
Implications for hospital managers and policy makers
If hospitals are to pursue the impressive productivity gains seen in aviation, they should follow a similar approach:
- Negotiate contracts, ideally digital contracts with real-time monitoring, that create shared incentives for hospitals to improve the efficiency of hospital care.
- Implement self-service digital scheduling for low-risk or routine clinic appointments to improve patient experience, reduce labor costs associated with scheduling, and deploy algorithms that incentivize patients to choose appointments that optimize hospital operational efficiency.
- Invest in integrated operational optimization that simultaneously considers how surgical blocks are scheduled, how surgical cases are scheduled into blocks, how services are assigned to hospital units, how hospital units are staffed, etc.
Healthcare organizations should expand their current focus on serial or local optimization efforts, e.g., improving single-unit nurse scheduling efficiency, to integrated or global efforts that encompass the entire value stream. The consideration of the value stream should start at the level of contracting, where digital contracts can be designed to reward hospitals for improving efficiency and lowering costs. Increased contractual clarity, e.g., real-time prior authorization can allow the expansion of self-service digital scheduling, pushing the work to consumers and increasing satisfaction. As aviation aggregators such as Kayak have driven transparency and competition in aviation, policymakers and regulators should push hospitals to allow innovative aggregators to optimize transparency for patients and encourage efficiency-driven hospital competition.
Limitations
Our analysis has several limitations. Productivity measurement in both industries involves methodological challenges, and the BLS measures are not perfectly comparable across sectors. Similarly, measuring hospitalization expenditures presents challenges that we do not consider and is typically done at the level of specific services or specialties. However, our findings are sufficiently high-level so as not to depend on the choice of a particular definition of cost. Our counterfactual analysis assumes without justification that hospitals could achieve significant savings, comparable to 50% of those seen in aviation, and that those savings would be passed on to consumers, the government, and insurers in the form of lower prices. Numerous factors independent of labor costs, such as prices negotiated with private insurance companies, drive hospital expenditures. This estimate should be considered as a point of reference rather than a rigorous finding. Finally, we do not account for quality differences — BLS hospital productivity measures include some quality adjustment, but the relationship between operational efficiency and care quality requires further study.
Conclusion
The productivity gap between airlines and hospitals represents one of the most significant and under-recognized opportunities to target reduced hospital savings. From 1995 to 2019, aviation labor productivity increased by 247% and prices declined by 28% while hospital labor productivity declined by 1% and per-capita expenditures increased by 287%. Technology-driven productivity improvements in hospital care, with a focus on strategies successfully deployed by airlines but not yet pursued by hospitals, require additional research.
References
- Centers for Medicare and Medicaid Services. National Health Expenditure Data. Accessed October, 2025. https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data
- Donaldson, M.S., Corrigan, J.M. and Kohn, L.T. eds., 2000. To err is human: building a safer health system.
- Rosko, M., Al-Amin, M. and Tavakoli, M., 2020. Efficiency and profitability in US not-for-profit hospitals. International Journal of Health Economics and Management, 20(4), pp.359-379.
- Sabel, J., 2004. Airline-airport facilities agreements: An overview. J. Air l. & Com., 69, p.769.
- Fu, X., Homsombat, W. and Oum, T.H., 2011. Airport–airline vertical relationships, their effects and regulatory policy implications. Journal of Air Transport Management, 17(6), pp.347-353.
- Karanki, F. and Lim, S.H., 2020. The effects of use agreements on airport efficiency. Journal of Air Transport Management, 84, p.101767.
- Harison, E. and Boonstra, A., 2008. Reaching new altitudes in e-commerce: Assessing the performance of airline websites. Journal of Air Transport Management, 14(2), pp.92-98.
- Williams, K., 2020. Dynamic airline pricing and seat availability.
- Arabeyre, J. P., Fearnley, J., Steiger, F. C., & Teather, W. (1969). The airline crew scheduling problem: A survey. Transportation Science, 3(2), 140-163.
- Barnhart, C., Belobaba, P., & Odoni, A. R. (2003). Applications of operations research in the air transport industry. Transportation Science, 37(4), 368-391.
- Gopalakrishnan, B., & Johnson, E. L. (2005). Airline crew scheduling: State-of-the-art. Annals of Operations Research, 140(1), 305-337.
- Anbil, R., Gelman, E., Patty, B., & Tanga, R. (1991). Recent advances in crew-pairing optimization at American Airlines. Interfaces, 21(1), 62-74.
- Xu, Y., Wandelt, S. and Sun, X., 2024. Airline scheduling optimization: literature review and a discussion of modelling methodologies. Intelligent Transportation Infrastructure, 3, p.liad026.
- Lohatepanont, M., & Barnhart, C. (2004). Airline schedule planning: Integrated models and algorithms for schedule design and fleet assignment. Transportation Science, 38(1), 19-32.
- Koos, H., Scheinker, D., Schulman, K. and Baker, L., 2025. Who Contracts on Diagnosis Related Groups and How Are They Priced? Evidence From Hospital Price Transparency. Health Services Research, p.e70059.
- Burke, E. K., De Causmaecker, P., Berghe, G. V., & Van Landeghem, H. (2004). The state of the art of nurse rostering. Journal of Scheduling, 7(6), 441-499.
- Hulshof, P. J., Kortbeek, N., Boucherie, R. J., Hans, E. W., & Bakker, P. J. (2012). Taxonomic classification of planning decisions in health care: A structured review. Health Systems, 1(2), 129-175.
- Dai, T. and Tayur, S., 2020. OM forum—Healthcare operations management: A snapshot of emerging research. Manufacturing & service operations management, 22(5), pp.869-887.
- Al Amin, M., Baldacci, R. and Kayvanfar, V., 2025. A comprehensive review on operating room scheduling and optimization. Operational Research, 25(1), p.3.
- Office of the National Coordinator for Health Information Technology. (2016). Hospital adoption of EHR technology. U.S. Department of Health and Human Services.
- O’Malley, A.S., 2011. Tapping the unmet potential of health information technology. N Engl J Med, 364(12), pp.1090-1091.
- Kellermann, A.L. and Jones, S.S., 2013. What it will take to achieve the as-yet-unfulfilled promises of health information technology. Health affairs, 32(1), pp.63-68.
- Bureau of Labor Statistics. New measure of labor productivity for private community hospitals: 1993–2012. Accessed October, 2025. https://www.bls.gov/opub/mlr/2015/article/new-measure-of-labor-productivity-for-private-community-hospitals-1993-2012.htm
- Bureau of Labor Statistics. Economic productivity in the air transportation industry: multifactor and labor productivity trends, 1990–2014. Accessed October, 2025. https://www.bls.gov/opub/mlr/2017/article/economic-productivity-in-the-air-transportation-industry.htm#edn2
- Bureau of Labor Statistics. Productivity. Accessed October, 2025. https://www.bls.gov/productivity/
- Bureau of Transportation Statistics. Air Fares. Accessed October, 2025. https://www.bts.gov/air-fares
- Staudenmayer, K., Stewart, C., Purvis, C. and Schulman, K., 2021. Innovations in technology: perspectives of hospital CIOs. Health Management, Policy and Innovation, 6(1).
- Government taps McKinsey to help manage $175 billion payout to hospitals. Accessed November, 2025. https://www.consulting.us/news/4410/government-taps-mckinsey-to-help-manage-175-billion-payout-to-hospitals
- Boston Consulting Group. Airline Industry. Accessed November, 2025. https://www.bcg.com/industries/travel-tourism/airline-industry