Tags: Policy Analysis
Alekhya Kommuru and Divyansh Agarwal, Stanford Graduate School of Business
Contact: div117@stanford.edu
Abstract
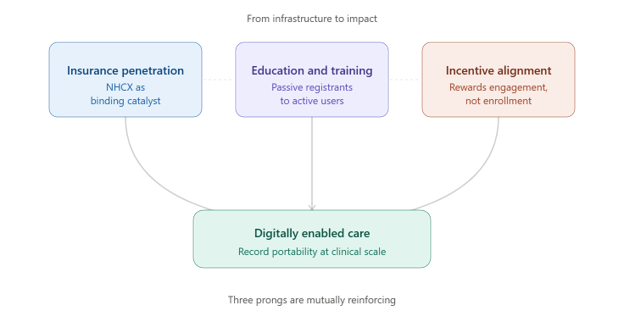
What is the message? India’s Ayushman Bharat Digital Mission (ABDM), launched in 2021, has built a foundational digital health infrastructure at unprecedented scale, with over 880 million unique health identifiers, 500,000+ registered facilities, and 1,000+ integrated private companies. Yet the pace of engagement has not been in line with enrolment: active record linkage and cross-facility retrieval remain far below the thresholds needed to generate clinical value. This paper argues that moving from infrastructure to impact requires a three-pronged approach: treating insurance penetration as the binding constraint and formalizing claims through National Health Claims Exchange (NHCX), investing in education and training to convert passive registrants into active users, and restructuring incentives through a combination of performance-linked payments and national mandate frameworks that close the gap between NHA’s convening role and the regulatory authority held by Insurance Regulatory and Development Authority of India (IRDAI) and the Ministry of Health and Family Welfare.
What is the evidence? Drawing on 15 primary interviews between January and March 2026 with ecosystem participants spanning government bodies, development organizations, digital health startups, and large healthcare companies, alongside government dashboard data and published literature, this paper examines adoption patterns across public and private sectors, presents case studies from multiple states illustrating diverse implementation paths, and identifies the structural incentive misalignments that constrain the transition to digitally enabled care in India.
Keywords: Digital Health, Health Policy
Timeline: Submitted May 25, 2026; accepted after review July 10, 2026.
Cite as: Alekhya Kommuru, Divyansh Agarwal. 2026. From Infrastructure to Impact: Operationalizing India’s Ayushman Bharat Digital Mission. Health Management, Policy and Innovation (www.HMPI.org). Volume 11, Issue 2.
Introduction
India’s healthcare system faces structural challenges of extraordinary scale. With a population of 1.4 billion, a doctor-to-patient ratio of approximately 1:1,000 nationally (dropping to 1:4,500 in rural areas), and out-of-pocket expenditures historically representing nearly half of total health spending, the gap between supply and demand cannot be addressed through incremental reform (1). The government of India recognized that technology would need to function as a structural solution rather than an administrative convenience.
The Ayushman Bharat Digital Mission (ABDM) was launched nationally in September 2021. Building on the India Stack, which comprises Aadhaar biometric identity for 1.4 billion people, the Unified Payments Interface (UPI), which processed 117 billion transactions in 2023, and the Jan Dhan financial inclusion program, ABDM sought to do for healthcare what UPI had done for payments: create a shared, interoperable infrastructure layer that reduces friction, enables private innovation, and makes longitudinal care coordination possible at population scale. (2,3)
A prior paper examined ABDM’s architecture and its foundations in India’s digital public infrastructure strategy. If you are new to ABDM and its components, we strongly suggest reading it first. (4) This paper examines what has happened since: how ABDM is being operationalized on the ground, what adoption patterns have emerged across public and private sectors, and what structural changes are needed to move from infrastructure to impact.
This paper draws on 15 semi-structured interviews conducted between January and March 2026 with participants across India’s public and private healthcare ecosystem. Interviewees included representatives from government bodies, development organizations, digital health startups, and large healthcare companies, spanning both frontline practitioners and central policy-level participants. Interview insights were synthesized through iterative discussion between the co-authors and reviewed by Professor Kevin Schulman, drawing on his expertise in digital health system design. These primary insights were triangulated against government dashboard data, peer-reviewed literature, and published policy documents throughout the analysis.
ABDM Architecture and Adoption
Architecture
ABDM’s architecture comprises five interconnected components: ABHA (Ayushman Bharat Health Account), a unique 14-digit health identifier; the Health Professional Registry (HPR); the Health Facility Registry (HFR); a patient-controlled personal health record (PHR) application; and the Unified Health Interface (UHI), an open protocol for healthcare transactions. Two critical gateways have since been added: NHCX (National Health Claims Exchange) for digital insurance claims processing, and the Health Information Exchange and Consent Manager (HIE-CM), which enables patients to grant and revoke consent for cross-facility data sharing. A defining architectural choice, federated rather than centralized storage, means patient data resides with facilities and is shareable with consent across the network, rather than aggregated in a central repository. (4)
As of May 2026, ABDM’s enrollment figures are substantial: 880+ million ABHA accounts, 500,000+ registered health facilities, and 860,000+ enrolled healthcare professionals. However, these figures require careful interpretation (5)(6). The CoWIN vaccination platform seeded approximately 130 million initial accounts without explicit separate consent, and Pradhan Mantri Jan Arogya Yojana (PM-JAY, a health insurance scheme offered by the Indian Government) integration has been the dominant driver of ABHA creation. A re-application anomaly, in which large numbers of duplicate creations appear in dashboard data, suggests the true denominator of unique active patients is materially lower than headline counts imply. (6)
ABDM distinguishes three engagement milestones: M1 (ABHA creation), M2 (record linkage within a facility), and M3 (cross-facility record retrieval). M1 has achieved mass scale. M2 activity is anchored to workflows like QR-based appointment check-in followed by prescription delivery to a health locker. M3, the milestone that would make ABDM genuinely valuable for care coordination, remains extremely low. This is the use case where the system’s full value lies: a patient presenting at a new facility can consent to share records from prior encounters, enabling a clinician to make informed decisions without redundant testing. (5) (6)
Adoption Challenges: Consent, Labs, and Pharmacies
The steepest drop-off in the ABDM adoption funnel occurs between M2 and M3. Based on research and interviews with people familiar with ground-level execution, the consent framework emerged as a persistent friction point. When a provider wishes to retrieve records from another facility, the patient must locate a notification in their PHR app, review time-bound consent parameters, and approve the request. In practice, this loop has proven difficult to close in high-volume settings: patients are frequently unaware that a notification has been sent, the interface presents a learning curve for first-time users, and in public hospitals that provide free diagnostics, clinicians often find it more expedient to reorder tests than to navigate the retrieval workflow. A promising design direction suggested by stakeholders is to simplify consent to a QR scan plus biometric or PIN confirmation at the point of care, analogous to a UPI transaction, while preserving the privacy safeguards that make the consent architecture trustworthy. The “Scan and Share” initiative has shown meaningful progress in reducing registration wait times, though implementation teams have noted a task-shifting dynamic at high-volume facilities where congestion, rather than eliminated, is redistributed to specialist referral desks.
Three broader implementation challenges compound these ground-level friction points. First, interoperability between ABDM’s open standards and the large installed base of legacy Hospital Management Information Systems remains unresolved. Many facilities run proprietary software with no ABDM-compliant API layer, and integration costs for mid-sized providers are estimated at INR 30-50 lakh. Second, provider workflow burden is a persistent barrier: ABDM’s value to the patient is real, but the workflow steps required of a physician during a two-to-five-minute consultation in a high-volume public facility can add time rather than save it. Third, data governance under the 2023 Digital Personal Data Protection Act (DPDPA) introduces compliance obligations like consent artifact storage, data localization requirements, and cross-entity sharing rules, all of which create legal uncertainty for private health technology companies building on ABDM infrastructure.
In the short term, labs and pharmacies provide a great opportunity to close this gap. However, laboratory adoption has been constrained by a circular incentive gap: incumbent Laboratory Management Information System (LMIS) vendors have been slow to build ABDM-enabled versions without demand from labs, while labs have had limited incentive to request integration without patient-side pull. Breaking this dynamic would bring diagnostic results into the ecosystem. Pharmacy integration presents a similarly clear pathway: a viable digital prescription-retrieval workflow would give pharmacies a meaningful role and create a natural forcing function for broader provider and patient engagement.
Multimodal State-Level Implementation
States have been leading the charge in deeper ABDM adoption and implementation. Across the 28 states and 8 union territories, three implementation archetypes have emerged, matching policy levers to local conditions. These archetypes are not mutually exclusive and several states show elements of more than one.
Private-Sector Engagement: Karnataka, Maharashtra, Gujarat
These states have a relatively concentrated urban private market and a vendor ecosystem that has built ABDM-compliant Hospital Management Information Systems (HMIS). Karnataka has achieved 93.9% Health Facility Registry (HFR) verification and meaningful engagement from private clinics and hospitals, supported by professional networks and targeted field engagement that generated trust signals cascading to smaller providers (7). Maharashtra’s Mumbai PATH pilot, IMA partnerships, and ward-level field teams have begun to onboard small clinics, although providers report few tangible incentives once field teams withdraw. Adoption in this archetype tends to begin with appointment booking and basic registration rather than full clinical record integration, and the model’s replicability is constrained by its dependence on concentrated urban markets (8).
Public-Infrastructure-Led: Tamil Nadu, Uttar Pradesh, Kerala, Rajasthan
Uttar Pradesh has rolled out Scan and Share at scale, with more than 22.7 million tokens issued, supported by IMA-UP WhatsApp peer groups and a strong state program management unit (9). Tamil Nadu has paired the Makkalai Thedi Maruthuvam (healthcare at your doorstep) community’s Non-Communicable Disease (NCD) outreach program with eSanjeevani, and is thus recording one of the highest volumes nationally (10). Kerala’s ‘eHealth Kerala’ UHID platform covers more than 600 institutions and leverages the highest level of frontline digital literacy in the country, but faces identifier friction between UHID and ABHA and uneven module adoption (11). Rajasthan’s iHMS auto-enrolls ABHA at the front desk, but an ABHA-to-EHR linkage rate of below 20% illustrates what happens when enrollment-oriented incentives are not balanced by usage-oriented accountability. The shared challenge across these states is that records are produced at outreach or front-desk events but are not consistently retrieved at subsequent facility visits.
Telemedicine-Integrated: Andhra Pradesh, Telangana, Madhya Pradesh
The shared anchor in this archetype is eSanjeevani teleconsultation at Ayushman Bharat Health and Wellness Centres (AB-HWC), where community health officers provide assisted consultations that generate ABHA-linked digital prescriptions. Andhra Pradesh and Telangana have built hub-and-spoke arrangements with ABHA-linked NCD screening, and Telangana reports more than 98% AB-HWC coverage (12) (13). Madhya Pradesh ranks among the top five contributor states nationally for eSanjeevani volumes (14). The model reaches populations that no self-service digital application could serve, but its characteristic failure mode is episodic value: teleconsultations produce records that are not consistently retrieved at subsequent in-person encounters, and the continuity loop that would make ABDM clinically meaningful for chronic disease management remains largely untapped. The digital divide here is a design constraint that requires workflow solutions, not just technology solutions.
Across all active archetypes, two patterns repeat: adoption begins at registration rather than at clinical record use, and engagement plateaus once field teams withdraw unless a downstream incentive sustains it.
The Way Forward: A Three-Pronged Approach
Based on our interviews with people closer to the ground and to the central policy level, and drawing learnings from research across similar globally successful models within healthcare, we suggest a three pronged approach to move ABDM from infrastructure to impact.
1. Insurance Penetration as the Binding Constraint
A central reason ABDM’s clinical value remains latent is that the underlying payment system does not yet reward digitization. India’s health spending is dominated by out-of-pocket payments at the point of care, roughly 48.8% of total health expenditure, against 40.8% government spending and only 5.8% private health insurance (8). When patients pay cash and providers maintain cash-based bookkeeping, neither side gains immediate value from electronic claims, structured records, or interoperable history.
This is why NHCX matters disproportionately. As insurance penetration rises, whether through PM-JAY expansion, employer-sponsored plans, or individual cover sold under IRDAI’s expanded mandates, the share of payments that must flow through a digital adjudication path grows. Each additional insurance-paid encounter is, by construction, an encounter that benefits from ABDM compliance: a digital claim, a structured discharge summary, and a verifiable record. The current cash dominance will loosen as insurance share rises, and we recommend directing policy levers at accelerating that shift.
ABDM’s most persistent structural challenge on the provider side is that integration requires upfront investment with uncertain commercial return and no regulatory mandate. For payers, NHCX offers a clear commercial incentive: digital claims processing reduces fraud, accelerates the approximately 45-day average settlement cycle, and lowers administrative costs. We recommend that IRDAI require all health-insurance claims above a defined threshold to be processed through NHCX within a fixed transition window, creating an immediate mandate for insurer participation and, by extension, pressure on empaneled facilities to comply. Making NHCX integration a condition for PM-JAY empanelment would create a mandate-adjacent incentive structure that drives provider-side adoption.
2. Education and Training
A substantial share of ABDM’s adoption gap is not technological but behavioral. Patients who have registered for ABHA do not understand what it does, providers who have onboarded facilities do not use digital workflows as part of the consultation, and frontline health workers who generate records through assisted channels are not trained to close the loop with patients on record retrieval. We recommend addressing this by investing across three levels.
At the patient level, the 880+ million individuals with ABHA accounts represent a registered population that has never been systematically informed about the value of their health account. We recommend a targeted national awareness program, delivered through Aarogya Setu, PM-JAY communications, and community health workers, to convert passive registrants into active PHR users.
At the provider level, the gap between facility registration and clinical workflow adoption is a training problem as much as an incentive problem. Short structured modules integrated into continuing medical education, focused on the three most common ABDM workflows (QR check-in, prescription push, and consent-based record retrieval) would reduce the friction that currently makes paper feel faster.
At the system level, community health officers at AB-HWCs, who are already the primary interface between ABDM and rural populations, need training on closing the post-visit loop: explaining to patients that their teleconsultation has generated a digital record, how to access it, and why it matters for their next encounter.
3. Incentive Alignment: Sticks, Carrots, and Mandates
The third prong addresses the structural reality that ABDM’s current incentive architecture rewards enrollment over engagement and leaves participation voluntary for actors whose involvement is necessary for the system to function. We propose action on both incentive reform and mandate mechanisms.
In terms of reforming existing incentives, one solution could be changing the INR 20 per ABHA payment structure to reward active record linkage rather than mere account creation. Performance-linked payments to facilities based on M2 and M3 transaction volumes, modeled on the incentive logic of PM-JAY empanelment payments, would shift provider behavior toward the outcomes that generate clinical value. For private health technology companies, a tiered compliance framework that provides preferential access to ABDM’s digital sandbox, faster certification timelines, and API rate allowances in exchange for demonstrated M3 transaction volumes would create a commercial reason to invest in the harder adoption problems.
Mandate mechanisms offer a complementary path and as discussed earlier, processing health insurance claims through NHCX and making ABDM compliance at M2 level a condition of PM-JAY empanelment, can be helpful levers. Besides these, the National Medical Commission, operating through state medical councils, could require HPR registration and verification as a precondition for license renewal, addressing the bottleneck that currently leaves a significant share of registered providers unverified and limiting the clinical trust that depends on a credible provider directory.
The National Health Authority is a convening and implementation body, not a regulator; it cannot, on its own authority, compel facilities or insurers to adopt the standards it publishes. Genuine adoption inflection will therefore require either NHA partnerships with regulators that already hold mandate authority, or a national-level mandate channeled through Parliament or the Cabinet. A national mandate framework that defines a minimum compliance floor while preserving state discretion over implementation is the policy architecture we propose.
Each of the above addresses a distinct failure mode in the current adoption trajectory, and the three are mutually reinforcing: progress on insurance penetration creates the financial incentive for providers to engage; education and training equips both patients and providers to use the system once the incentive exists; and incentive alignment through government policy ensures the system does not remain voluntary for actors whose participation is structurally necessary.
Lastly, two segments — labs and pharmacies — offer a near-term opportunity to accelerate this dynamic without waiting for broader mandate frameworks. We recommend targeted API support and onboarding incentives directed at LMIS vendors, combined with a viable digital prescription-retrieval workflow for pharmacies, to bring diagnostic results and medication records into the ecosystem and create natural forcing functions for both provider and patient engagement.
Conclusion
ABDM represents a genuine architectural achievement. In five years, India has built the infrastructure for a federated digital health ecosystem at a scale no comparable country has achieved. The central challenge is now the transition from infrastructure to impact, a transition that requires behavioral change among all ecosystem stakeholders, each operating under different incentive structures. The history of digital health implementation globally, from HITECH in the United States to NHS Digital in the United Kingdom, suggests that infrastructure build-out is the easier part. Adoption is harder, and clinical impact is hardest of all.
The three-pronged approach outlined above addresses each of the structural failure modes that currently prevent ABDM from delivering clinical value at scale. None of these interventions is technically complex; all of them require political will and cross-institutional coordination. It’s also important to mention here that ABDM is ultimately intended to address the provider shortage in India through the development of a platform for digital services for patients. M2/M3 data exchange should be seen as the prerequisite building blocks of these high-quality services, not as the destination for the program. India’s extraordinary physician shortage means the value of longitudinal records, which enable a stretched clinical workforce to deliver more effective care in shorter encounters, is higher here than almost anywhere. The architecture exists. The task now is activation.
References
- World Bank. “Out-of-Pocket Expenditure (% of Current Health Expenditure) – India.” World Bank Open Data. Accessed May 10, 2026.
- National Payments Corporation of India. UPI Product Statistics. NPCI.
- Government of India. PM Jan Dhan Yojana. PMJDY. https://pmjdy.gov.in/ (2021).
- Narayan A, Bhushan I, Schulman K. India’s evolving digital health strategy. npj Digital Medicine. 2024;7:284.
- Ayushman Bharat Digital Mission, “ABDM-Insights,” accessed May 13, 2026, https://dashboard.abdm.gov.in/abdm/
- Mishra, Udaya Shankar, Suryakant Yadav, and William Joe. “The Ayushman Bharat Digital Mission of India: An Assessment.” Health Systems & Reform 10, no. 2 (2024): 2392290. https://doi.org/10.1080/23288604.2024.2392290.
- Business Standard, October 2, 2024; https://www.business-standard.com/india-news/karnataka-tops-in-verified-health-facility-registry-tn-odisha-at-bottom-124100200701_1.html
- Kaul, Varun, and Tanu Gupta. “Private Sector Engagement for Digitizing Health Care in India.” PATH, March 22, 2023.
- NITI for States – UP best practices document on Scan and Share and HMIS
- BMC Primary Care peer-reviewed study, Dec 2025; https://link.springer.com/article/10.1186/s12875-025-03064-w
- Discover Public Health peer-reviewed study, Jul 2025; https://link.springer.com/article/10.1186/s12982-025-00829-7
- PMC study (Sood et al., 2025, Oxford Open Digital Health); https://pmc.ncbi.nlm.nih.gov/articles/PMC12558045/
- PIB press release; https://www.pib.gov.in/PressReleasePage.aspx?PRID=1830743
- NFHS-5 (National Family Health Survey 2019-21)
Other sources
- Press Information Bureau of India. NHA and C-DAC Launch e-Sushrut HMIS. PRID=2156603. January 2026.
- Ministry of Health and Family Welfare. eSanjeevani. esanjeevani.mohfw.gov.in. Accessed 2024.
- Government of India. Digital Personal Data Protection Act 2023. Ministry of Electronics and Information Technology, 2023.
- Narayan A, Schulman K. Access Health India and the Ayushman Bharat Digital Mission. Stanford GSB Case SM-359. 2022.
- Wood S, Rosengaus L, Thompson R, Patel K, Schulman K. The Digitally Enabled Care Framework: Leveraging Technology to Enhance the Physician-Patient Relationship. NEJM Catalyst Innovations in Care Delivery. 2024;5(10).
Acknowledgements
The authors conducted over 15 interviews for this research across India’s public and private healthcare ecosystem, from frontline practitioners to state and central policy makers, from start founders to large health system executives. We thank all our interviewees for their time and candid feedback. We also have deep gratitude to Professor Kevin Schulman (Stanford University) for this support, insights and guidance throughout this journey. Interviews were conducted between January and March 2026. No specific funding was received for this work.