Tags: Practitioner Perspective
Irene Afua Quarshie, QL Consulting, and K. Davina Frick, Johns Hopkins University
Contact: iquarshie@qlconsultinggroup.com
Abstract
What is the message? FemTech innovations deliver maximum value when evaluated through a life course framework that provides integrated, longitudinal care across women’s interconnected health needs. This transforms women’s health from a siloed initiative into a strategic business lever for health systems, payers, and employers.
What is the evidence? The analysis demonstrates that despite historical neglect leaving women spending 25% more of their lives in poor health, the rapidly growing FemTech market ($60 billion projected by 2027) shows measurable returns on investment: improved workforce participation, enhanced value-based care metrics, and workforce retention when innovations – from menstrual health apps to digital menopause solutions – are implemented across key life stages.
Timeline: Submitted: April 3, 2025; accepted after review October 3, 2025.
Cite as: Irene Afua Quarshie, K. Davina Frick. 2025. Toward a Life Course Model of Innovation: FemTech and the New Health Economy. Health Management, Policy and Innovation (www.HMPI.org). Volume 10, Issue 2.
The Untapped Potential of Women’s Health Innovation
For decades, women’s health has been systematically sidelined in research and innovation (1). This neglect has materialized in tangible ways: women spend 25% more of their lives in substandard health compared to men (2), a disparity that carries significant costs for individuals, employers, and the healthcare system. The economic consequences are staggering, with estimates suggesting that addressing these gender-based disparities could add up to $1 trillion to the global economy by 2040 (2).
The root of this gap lies in a history of structural exclusion where formal policies and deeply ingrained societal norms reinforced one another (1). Menstruation, menopause, and fertility have been enveloped in taboo, leading to their marginalization (3). This societal posture, which often viewed the female body as overly complex or simply through the lens of reproductive risk, provided a rationale for codifying this exclusion into policy (3). A case in point is the 1977 FDA guideline which formally excluded women of childbearing capacity from phase 1 and early phase 2 clinical trials until teratogenicity studies in animals were completed and effectiveness was established in either men, older women or both – an action intended to be protective, yet exclusionary (4).
In some instances, this pattern of exclusion was not driven solely by protective concerns; it was also rooted in flawed scientific convenience and outright bias (4). For instance, a 1970 study to examine the effects of estrogen on preventing secondary cardiovascular disease in postmenopausal women focused exclusively on males, with researchers justifying the choice by arguing that the hormonal fluctuations in women would complicate the analysis (2) – an assumption as untested as the intervention itself. This was not an isolated occurrence. Instead, it illustrated a more extensive pattern of systematic exclusion. Together, these examples illustrate a pervasive and systematic exclusion that created a healthcare system designed, by default, around a male model, leaving critical gaps in our understanding of female-specific conditions and sex-based biological differences (2,5).
This history of neglect makes the rare moments of progress all the more telling. Landmark developments, such as the introduction of the contraceptive pill and the pap smear, demonstrate the immense potential that can be unlocked when innovation is focused on women’s health. The contraceptive pill did so much more than grant reproductive autonomy; according to Nobel Peace Laureate Claudia Goldin, it was one of the major disruptors of the modern labor market (6). Additionally, the pap smear did more than just detect abnormal cells; it revolutionized the very concept of preventative medicine (7), establishing the world’s first successful mass cancer screening program. By demonstrating that cancer could be detected at a precancerous stage, it laid the foundation for contemporary preventive oncology and shifted the primary focus of medicine from treatment to prevention.
These advancements are not merely exceptions to the rule of neglect; they are proof of the transformative power of investing in women’s health. Yet, they have remained the exception, not the rule. Pervasive gaps in women’s health persist today, fueled by a continuing lack of gender-disaggregated data and a legacy of underfunding that hinders research and development (R&D) and impairs healthcare delivery systems (2).
The Landscape of Women’s Health: Unmet Needs & Market Gaps
In response to these deep-seated challenges, a new industry, appropriately named FemTech (Female Technology), has emerged to meet demand. FemTech is the subdivision of the medical device industry that focuses on building devices, software applications, and providing services specific to female health care (8). FemTech was coined in 2016 by Ida Tin, co-founder of the fertility-tracking app Clue. She reasoned that a unique term for this industry would legitimize the female health tech market and remove the stigma that still frequently surrounds conversations around topics such as menstruation (9).
Despite evidence that innovation improves patient and healthcare system outcomes, women’s health has not advanced much since it has generally been viewed as a niche medtech market (8). While the term “niche” may allude to a special segment, it is frequently incorrectly associated with a small audience. This characterization of FemTech is therefore misleading: while women’s health may require specialized approaches, it in no way represents a small market opportunity.
Quite to the contrary: FemTech is a rapidly expanding market with immense potential, propelled by technical developments, greater awareness and ventures frequently led by female entrepreneurs. By 2027, this market is expected to generate $60 billion in revenue (10). Beyond gynecologic care, this field of medical technology covers a wide range of women’s health needs, including wearable sensors for pregnancy and hormone monitoring, telemedicine platforms for specialized women’s health consultations, digital therapeutics for conditions like endometriosis and mental health, mobile applications for fertility tracking and symptom management, and diagnostic hardware like portable ultrasound and screening devices (11).
The Life Course Perspective
The life course perspective offers a robust conceptual model for understanding the relationship between women’s health and innovation. According to the World Health Organization, the life course perspective (or life course theory) is a multidisciplinary approach to understanding the mental, physical and social health of individuals (12). In this context, it recognizes that women’s health challenges are not discrete occurrences. Rather, they are shaped by a complex interaction of physiologic, social, and economic elements that evolve across various life stages. And each of these stages – menstruation, pregnancy, menopause, and the management of chronic conditions – affects women’s well-being, workforce participation, career progression, and economic productivity (8).
Building on this understanding, the life course framework is particularly helpful in addressing the inclination to restrict women’s health solely to reproductive events such as childbirth, abortion and contraception. As Mishra et al. (13) argue, when these experiences are treated as isolated episodes rather than connected milestones, care becomes fragmented and ignores women’s long-term health trajectories. The framework challenges this fragmentation by demonstrating the connections between reproductive events and the subsequent risk of chronic disease later in life. Instead of treating women’s needs in discrete silos, it reframes reproductive health as a component of a continuum across the lifetime, emphasizing the need for innovations that support a more integrated and longitudinal model of care.
Women’s health needs are inextricably linked to workforce participation and economic systems (14). Reproductive health frequently overlaps with critical career milestones, influencing decisions around education and employment (6). Pregnancy and maternal health often precipitate challenges in the workplace, where mothers can face biases regarding their competence and commitment that affect hiring and compensation (15). As women age, menopause and age-related health needs can impact career longevity by creating notable retention challenges, with studies showing that many women consider leaving the workforce due to their symptoms (16).
However, these health needs remain inadequately addressed by both workplace policy and the innovation of FemTech solutions (1). The situation is further complicated by chronic health conditions, such as autoimmune diseases and mental health disorders, which add another layer to women’s health needs.
Beyond social and economic factors, sex-based biological differences introduce another dimension to women’s health, particularly in how diseases present and progress. Cardiovascular disease offers a clear example: women often present with non-specific symptoms for myocardial infarction (MI), have a higher mortality rate within a year of an MI, and typically develop Coronary Artery Disease (CAD) 10 to 15 years later than men (17).
These interrelated health themes underscore a clear need for integrated solutions that support women’s health across the full arc of their lives and enable their full participation in the economy.
Figure 1: A framework showing internal and external factors that impact the health of women across the lifespan. Adapted from the extended NIH ORWH multidimensional framework (1).
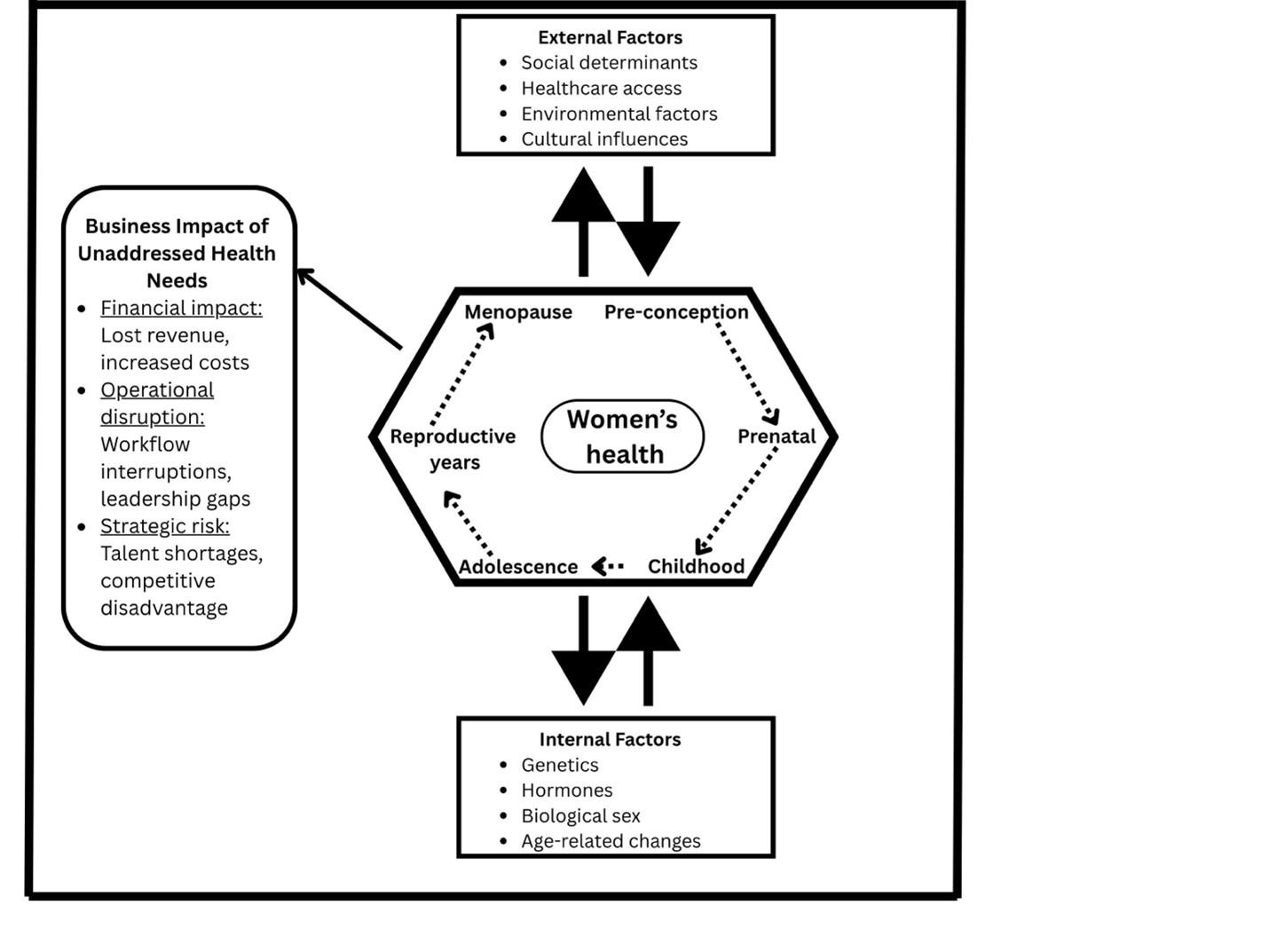
For healthcare managers, the life course perspective offers a way to reframe women’s health, shifting the focus from an episodic cost center to a continuous, quality-enhancing service line with long-term value. This shift in perspective provides a strategic lens for addressing the financial, operational, and competitive challenges that define success in modern healthcare markets.
The Managerial Case for Life Course FemTech Investment
Why Fragmented Approaches Fail: The Hidden Costs of Episodic Women’s Health
Healthcare systems organized around discrete episodes rather than longitudinal women’s health management, miss critical opportunities to prevent costly chronic conditions, as evidenced by the $350 billion annual cost of treating chronically ill women in the United States (18). This presents a fundamental issue for healthcare administrators working under value-based care contracts. The life course perspective explains why fragmented methods lead to cascading expenses that reduce profits and compromise patient experience and hospital quality ratings.
Consider the total financial impact of untreated Polycystic Ovary Syndrome (PCOS), a condition affecting women of reproductive age with a pooled mean prevalence of 21.27% (19). A 31-year-old woman with PCOS receives fragmented therapies under an episodic care approach, including sporadic gynecological appointments, emergent contraceptive consultations, and reproductive treatments. This fragmented approach creates poor patient experiences characterized by disruptions in treatment, and a lack of time and attention to patient concerns (20). According to Rubin et al. (21), PCOS patients are four times more likely than controls to develop type 2 diabetes. This amounts to a total economic burden of $4.36 billion annually in the United States, with costs spanning initial evaluation ($93 million), hormonal treatment for menstrual dysfunction ($1.35 billion), infertility care ($533 million), PCOS-associated diabetes ($1.77 billion), and hirsutism treatment ($622 million) (22).
The fragmentation that characterizes traditional women’s health services (23), is addressed by comprehensive FemTech platforms. At the population level, this coordinated approach becomes essential for health systems managing thousands of women with PCOS under value-based contracts.
Strategic Investment Framework: High-Impact FemTech Categories
Considering the investment priorities of healthcare managers – measurable returns and alignment with value-based care objectives – this analysis identifies three high-impact FemTech categories that deliver quantifiable financial and operational benefits.
Maternal Health Technology: The Highest-Return Investment
The strongest commercial case for FemTech investment is in maternal health, where evidence suggests mHealth interventions may be cost-effective, particularly those featuring notifications, reminders, and personalized health education. Pregnancy is a crucial time frame during which treatments may be used to enhance health outcomes and provide long-term advantages (24).
One example of the direct impact of FemTech investment is remote patient monitoring for postpartum hypertension. In contrast to standard care, which had 33% and 70% compliance rates among Black and non-Black women, respectively, Penn Medicine’s text-based blood pressure monitoring program had >90% compliance rates in both groups. While there were four readmissions in the standard care group, the remote monitoring technology completely avoided readmissions (25). For health systems addressing maternal health disparities, this text-based approach not only improves clinical outcomes but also reduces costly readmissions while ensuring equitable care delivery. The integration of comprehensive maternal health platforms can address several value-based care needs (25) by enabling early identification of high-risk patients (26) through combined clinical and socioeconomic risk assessment (27).
The benefits of employee retention generate value that is sometimes disregarded in conventional ROI calculations. Research demonstrates that family-supportive policies, including maternal health initiatives, can help organizations retain women by reducing perceptions of discrimination and subsequent turnover decisions (28). This is particularly relevant given that over 60% of healthcare employees are women and nurses comprise more than 80% women in provider organizations (29). Healthcare organizations must invest substantial resources to advertise, recruit, hire, and train new nurses to replace those who resign, while also losing intellectual capital and productivity (30). Given that nurse turnover costs range from $21,514 to $88,000 per nurse in the United States (30), comprehensive maternal health benefits could serve as a cost-effective retention strategy that simultaneously enhances employee satisfaction and patient care quality.
Menopause Management: Addressing Peak Career Impact
Menopause management represents an underrecognized investment opportunity with significant implications for workforce productivity, patient satisfaction, and long-term health outcomes. Comprehensive FemTech solutions have the potential to be more cost-effective than episodic care at addressing the unique issues created by the confluence of biological changes with peak earning years, especially considering the significant economic losses from untreated menopausal symptoms and the underdeveloped nature of this market.
Menopause affects 20% of the US workforce and causes a 10% drop in earnings four years after diagnosis. This makes menopause management an underappreciated investment opportunity with substantial impact on workforce productivity (31). The combination of biological changes and peak earning years results in economic losses equivalent to job displacement (31) with women becoming 4.8 percentage points more likely to obtain disability insurance and leave the workforce earlier. Comprehensive FemTech solutions that increase access to care show quantifiable cost-effectiveness; women who receive more therapy report lower earnings losses and improved labor market outcomes (31). Digital menopause platforms offer hormone optimization, symptom management, and lifestyle coaching.
The long-term health impacts enhance value under risky contracts. According to Hodis and Mack, hormone replacement treatment started within 10 years of menopause lowers coronary heart disease by 32% and all-cause mortality by 39% (32) with some studies reporting even higher reductions. While targeted osteoporosis treatments like raloxifene can reduce vertebral fractures by up to 40% (33), standard-dose hormone therapy reduces hip fractures by 28% and vertebral fractures by 35% (33). Early intervention through comprehensive menopause management, including appropriately timed hormone optimization, bone health monitoring, and cardiovascular risk assessment, represents a high-value intervention that delivers quantifiable health outcomes and supports long-term workforce productivity. Geriatric hip fractures cost an average of $13,113 per episode (34), while individuals with coronary artery disease may cost up to $150,000 in healthcare over the course of their lifetimes (35). These substantial downstream costs make fracture prevention and cardiovascular risk reduction through comprehensive menopause management a high-value intervention.
Chronic Condition Management: Preventing High-Cost Complications
Uterine fibroids exemplify the financial burden of fragmented chronic condition management. In 2003, uterine fibroid treatments represented over $1.5 billion in national hospital costs, with hysterectomies accounting for the majority of cases and individual procedures averaging $6,364 per patient (36). The most common surgical procedure, total abdominal hysterectomy, averaged 2.9 days length of stay with mean costs of $6,331, while laparoscopically assisted vaginal hysterectomy had the highest costs at $7,108, despite shorter stays. These figures, representing only inpatient costs without accounting for outpatient management, specialist consultations, and productivity losses, underscore the substantial economic impact of conditions affecting millions of women.
The pattern repeats across other women’s chronic conditions. Endometriosis, affecting 10% of women of reproductive age, demonstrates the financial consequences of delayed diagnosis and fragmented care (37). Diagnosis takes an average of 4.4 years, during which patients accumulate $2,801 per year in direct healthcare costs through multiple specialist appointments, emergency visits, and unsuccessful treatments, plus an additional $1,023 in productivity losses (37,38). FemTech solutions like Phendo and Syrona Health address these inefficiencies through AI-powered symptom tracking, lifestyle modifications, and coordinated care pathways designed to enable earlier diagnosis and comprehensive symptom management.
Mental health integration across women’s health conditions delivers additional value through improved care coordination and medication adherence, reducing crisis interventions and emergency utilization while improving patient outcomes. Health systems that successfully implement comprehensive chronic condition management platforms can expect measurable reductions in emergency department visits, decreased specialist referral patterns, and improved patient satisfaction scores alongside the direct cost savings from preventing high-cost complications.
Implementation Strategy: Metrics-Driven Deployment
For FemTech to be implemented successfully, measuring frameworks must be methodical and compatible with current financial management and quality reporting systems. Clear performance metrics that satisfy payer standards and regulatory compliance are essential for healthcare management board members, medical directors, and CFOs.
Financial Metrics and ROI Tracking
Implementing life course FemTech solutions requires robust financial tracking that records both potential revenue enhancement and immediate cost reductions. Key performance indicators(KPIs) should include ED utilization rates, hospital readmission rates, trends in specialist referrals, and costs associated with chronic care management. Since value-based care agreements usually monitor outcomes-based metrics like readmissions and ED utilization, these metrics are in perfect alignment with the requirements of value-based care contracts (39). These metrics provide clear evidence of investment returns while supporting quality reporting requirements.
Maternal health platforms demonstrate measurable impact through key metrics including cesarean section rates, NICU admissions, postpartum readmissions, and breastfeeding success rates. These metrics provide clear ROI calculations through direct correlations with quality and cost scores, enabling health systems to track substantial improvements and cost savings.
Medication adherence rates, trends in emergency department utilization, specialist visits, and patient-reported outcome indicators should be the main emphasis of tracking. Digital platforms enhance these measures for disorders like PCOS and endometriosis, with financial benefits recognized when improved continuous care prevents downstream consequences.
Quality and Patient Experience Integration
FemTech implementation must align with existing quality measurement programs, including HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores, CMS star ratings, and specialty-specific quality metrics. These platforms can enhance care coordination and access to specialized women’s health services, potentially improving competitive positioning in consumer choice marketplaces and supporting performance under value-based purchasing programs. Patient engagement metrics offer leading indicators of long-term performance: monitoring patient-reported outcomes, care plan adherence, and app usage offers early warning systems for program optimization and modification. Provider satisfaction represents another crucial area of evaluation. Digital health solutions in maternal care, including telemedicine interventions and remote monitoring, have demonstrated high provider satisfaction through time savings, reduced administrative burden, and improved care efficiency (40). These improvements may correlate with reduced physician turnover and enhanced recruitment capabilities.
Population Health and Risk Stratification
Life course FemTech uses risk categorization and ongoing monitoring to provide population health management. Rich data streams produced by platforms can identify high-risk individuals before urgent treatments are required. Under capitated contracts, where early intervention avoids costly complications, this capability is advantageous.
Risk stratification algorithms integrated into comprehensive FemTech systems can identify individuals at high risk of developing menopausal complications, postpartum depression, or gestational diabetes before they manifest clinically. Predictive analytics enable health systems to make proactive decisions about patient care and inclusion using historical data by identifying nuanced criteria for early intervention (39).
Data analytics skills enhance population health reporting and regulatory compliance by automating the monitoring of social determinants of health effects and health disparities, while facilitating community health needs assessment reporting, adherence to the Healthcare Effectiveness Data and Information Set (HEDIS), and health equity programs.
Competitive Advantage and Market Positioning
The strategic implementation of life course FemTech creates sustainable competitive advantages that extend beyond immediate financial returns.
Comprehensive women’s health programs are patient attraction and retention tools, especially given women’s active roles in family healthcare decisions. Health systems that demonstrate genuine commitment to women’s longitudinal health needs can capture disproportionate market share in family healthcare decisions. Market differentiation with cutting-edge FemTech products puts health systems at the forefront of technology while meeting patient expectations for accessible care. Integrated platforms that transition seamlessly from pregnancy care to pediatrics to women’s primary care create “sticky” relationships that are likely to generate higher patient lifetime value through continued engagement. Brand positioning around innovations in women’s health creates value through favorable press coverage and opportunities for community engagement. By putting comprehensive FemTech strategies in place, health systems could experience benefits in brand perception and market positioning that help with patient acquisition and community engagement.
Strategic FemTech investment represents a fundamental shift from reactive, episodic women’s health services toward proactive, longitudinal health management. Comprehensive women’s health efforts generate quantifiable results while addressing various strategic objectives for healthcare leaders navigating workforce challenges, value-based care transitions, and competitive pressures. The business case is based on proven gains in clinical outcomes, operational effectiveness, and financial performance – all of which characterize organizational success in contemporary healthcare markets – and the life course perspective offers the foundation for comprehending this potential.
References
- White J, Clayton J. The gender health innovation gap: A perspective from the NIH Office of Research on Women’s Health. Med. 2022;3(5):298-301. https://doi.org/10.1016/j.medj.2022.04.010
- Moley K. Closing the gender health gap is a $1 trillion opportunity. Biopharma Dealmakers. 2024. https://doi.org/10.1038/d43747-024-00021-x
- Babbar K. Taboos and myths as a mediator of the relationship between menstrual practices and menstrual health. European Journal of Public Health. 2021;31(Supplement_3):ckab165-552.
- Mazure CM, Jones DP. Twenty years and still counting: Including women as participants and studying sex and gender in biomedical research. BMC Women’s Health. 2015;15(1):1-16. https://doi.org/10.1186/s12905-015-0251-9
- Sherman LA, Temple R, Merkatz RB. Women in Clinical Trials: An FDA Perspective. Science. 1995;269(5225):793-795. https://doi.org/10.1126/science.7638593
- Goldin C, Katz LF. The Power of the Pill: Oral Contraceptives and Women’s Career and Marriage Decisions. Journal of Political Economy. 2002;110(4):730-770. https://doi.org/10.1086/340778
- World Health Organization. Comprehensive cervical cancer control: A guide to essential practice. 2nd ed. Geneva: World Health Organization; 2014. https://iris.who.int/handle/10665/144785
- Warty RR, Smith V, Patabendige M, Fox D, Mol B. Clarifying the unmet clinical need during medical device innovation in women’s health – A narrative review. Health Care for Women International. 2024;45(7):811-839. https://doi.org/10.1080/07399332.2023.2190983
- Wiederhold BK. Femtech: Digital Help for Women’s Health Care Across the Life Span. Cyberpsychology, Behavior, and Social Networking. 2021;24(11):697-698. https://doi.org/10.1089/cyber.2021.29230.editorial
- Emergen Research. Femtech Market By Type, By End-Use, By Application, By Region, Forecasts to 2027. 2020. https://www.emergenresearch.com/industry-report/Femtech-market
- Farahani NZ, Faubion S, Sundsbak J, Bethke S, Enayati M. Femtech Solutions and Devices: Technological Innovations and their Impact on Women’s Health Outcomes. In: Frontiers in Biomedical Devices. Vol 88735. American Society of Mechanical Engineers; 2025. p. V001T09A014.
- Elder GH, Johnson MK, Crosnoe R. The Emergence and Development of Life Course Theory. In: Mortimer JT, Shanahan MJ, editors. Handbook of the Life Course. New York: Springer US; 2003. p. 3-19. https://doi.org/10.1007/978-0-306-48247-2_1
- Mishra GD, Cooper R, Kuh D. A life course approach to reproductive health: Theory and methods. Maturitas. 2010;65(2):92-97. https://doi.org/10.1016/j.maturitas.2009.12.009
- Onarheim KH, Iversen JH, Bloom DE. Economic Benefits of Investing in Women’s Health: A Systematic Review. PLoS ONE. 2016;11(3):e0150120. https://doi.org/10.1371/journal.pone.0150120
- Correll SJ, Benard S, Paik I. Getting a job: Is there a motherhood penalty? American Journal of Sociology. 2007;112(5):1297-1338.
- Atkinson C, Beck V, Brewis J, Davies A, Duberley J. Menopause and the workplace: New directions in HRM research and HR practice. Human Resource Management Journal. 2021;31(1):49-64. https://doi.org/10.1111/1748-8583.12294
- Zhang Y, Liu B, Zhao R, Zhang S, Yu XY, Li Y. The influence of sex on cardiac physiology and cardiovascular diseases. Journal of Cardiovascular Translational Research. 2020;13(1):3-13.
- Gevirtz F, Corrato RR, Chodoff P, Nash DB. Chronic disease, women’s health, and “disease management”: The latest trend? Women’s Health Issues. 1999;9(1):18-29. https://doi.org/10.1016/S1049-3867(98)00036-X
- Deswal R, Narwal V, Dang A, Pundir CS. The Prevalence of Polycystic Ovary Syndrome: A Brief Systematic Review. Journal of Human Reproductive Sciences. 2020;13(4):261. https://doi.org/10.4103/jhrs.JHRS_95_18
- Jain T, Mudliar P. Platforming PCOS Treatment Online: Femtech Logics of Care. Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 2024:1-18. https://doi.org/10.1145/3613904.3642882
- Rubin KH, Glintborg D, Nybo M, Abrahamsen B, Andersen M. Development and risk factors of type 2 diabetes in a nationwide population of women with polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism. 2017;102(10):3848-3857.
- Azziz R, Marin C, Hoq L, Badamgarav E, Song P. Health Care-Related Economic Burden of the Polycystic Ovary Syndrome during the Reproductive Life Span. The Journal of Clinical Endocrinology & Metabolism. 2005;90(8):4650-4658. https://doi.org/10.1210/jc.2005-0628
- Elf M, Flink M, Nilsson M, Tistad M, von Koch L, Ytterberg C. The case of value-based healthcare for people living with complex long-term conditions. BMC Health Services Research. 2017;17(1):24. https://doi.org/10.1186/s12913-016-1957-6
- Carrandi A, Hu Y, Karger S, Eddy KE, Vogel JP, Harrison CL, Callander E. Systematic review on the cost and cost-effectiveness of mHealth interventions supporting women during pregnancy. Women and Birth. 2023;36(1):3-10.
- Triebwasser JE, Janssen MK, Hirshberg A, Srinivas SK. Successful implementation of text-based blood pressure monitoring for postpartum hypertension. Pregnancy Hypertension. 2020;22:156-159. https://doi.org/10.1016/j.preghy.2020.09.001
- McWilliams JM, Schwartz AL. Focusing on High-cost Patients: The Key to Addressing High Costs? The New England Journal of Medicine. 2017;376(9):807-809. https://doi.org/10.1056/NEJMp1612779
- Improving Risk Stratification Using AI and Social Determinants of Health. The American Journal of Managed Care. 2022;28(11):582-587. https://doi.org/10.37765/ajmc.2022.89261
- Paustian-Underdahl SC, Little LM, Mandeville AM, Hinojosa AS, Keyes A. Examining the role of maternity benefit comparisons and pregnancy discrimination in women’s turnover decisions. Personnel Psychology. 2024;77(2):819-846. https://doi.org/10.1111/peps.12577
- Berlin G, Darino L, Greenfield M, Starlkova I. Women in the healthcare industry. McKinsey & Company; 2019. https://hbanet.org/sites/default/files/2023-06/Women-in-the-healthcare-industry_Aug.2019.pdf
- Bae SH. Noneconomic and economic impacts of nurse turnover in hospitals: A systematic review. International Nursing Review. 2022;69(3):392-404. https://doi.org/10.1111/inr.12769
- Conti G, Ginja R, Persson P, Willage B. The menopause “penalty”. NBER Working Paper No. 33621. National Bureau of Economic Research; 2025. http://www.nber.org/papers/w33621
- Hodis HN, Mack WJ. Menopausal Hormone Replacement Therapy and Reduction of All-Cause Mortality and Cardiovascular Disease: It Is About Time and Timing. The Cancer Journal. 2022;28(3):208-223. https://doi.org/10.1097/PPO.0000000000000591
- Yong EL, Logan S. Menopausal osteoporosis: Screening, prevention and treatment. Singapore Medical Journal. 2021;62(4):159-166. https://doi.org/10.11622/smedj.2021036
- Denis A, Montreuil J, Bouklouch Y, Reindl R, Berry GK, Harvey EJ, Bernstein M. Hospital episode-of-care costs for hip fractures: An activity-based costing analysis. OTA International. 2023;6(4). https://doi.org/10.1097/OI9.0000000000000295
- Walker S, Asaria M, Manca A, Palmer S, Gale CP, Shah AD, Abrams KR, Crowther M, Timmis A, Hemingway H, Sculpher M. Long-term healthcare use and costs in patients with stable coronary artery disease: A population-based cohort using linked health records (CALIBER). European Heart Journal – Quality of Care and Clinical Outcomes. 2016;2(2):125-140. https://doi.org/10.1093/ehjqcco/qcw003
- Becker ER. National trends and determinants of hospitalization costs and lengths-of-stay for uterine fibroids procedures. Journal of Health Care Finance. 2007;33(3):1-16.
- Simoens S, Hummelshoj L, D’Hooghe T. Endometriosis: Cost estimates and methodological perspective. Human Reproduction Update. 2007;13(4):395-404. https://doi.org/10.1093/humupd/dmm010
- Soliman AM, Fuldeore M, Snabes MC. Factors Associated with Time to Endometriosis Diagnosis in the United States. Journal of Women’s Health. 2017;26(7):788-797. https://doi.org/10.1089/jwh.2016.6003
- Adams KM, Engelhardt NF. Strategic planning, goal setting, and marketing. In: Fitzpatrick JJ, Alfes CM, editors. Nurse leadership and management: Foundations for effective administration. 2022. p. 173-179.
- Hod M, Divakar H, Kihara AB, Geary M. The Femtech revolution – A new approach to pregnancy management: Digital transformation of maternity care – The hybrid e-health perinatal clinic addressing the unmet needs of low- and middle-income countries. International Journal of Gynecology & Obstetrics. 2023;163(1):4-10. https://doi.org/10.1002/ijgo.15032