Tags: Case Study
Melissa Dzinoreva, School of Medicine, Stanford University, Nicole D’Andrea, Carteret OB-GYN, James Whiteside, Eastern Carolina University, Brody School of Medicine, and Kevin Schulman, School of Medicine and Graduate School of Business, Stanford University
Contact: kevin.schulman@stanford.edu
Abstract
What is the message? As maternity care deserts expand across the United States, rural communities face an alarming decline in access to essential obstetric services. This paper presents a case study of Carteret County, North Carolina, a community at imminent risk of becoming a maternity care desert, and underscoring the urgent need for coordinated policy interventions, workforce support, and sustainable reimbursement models to safeguard maternal and infant health in vulnerable regions.
What is the evidence? An analysis of state-level maternal health trends, the operations of Carteret OB-GYN, and the broader healthcare infrastructure, highlight how workforce shortages, financial instability, and systemic mis-investment threaten the continuity of maternity care.
Timeline: Submitted: September 22, 2025; accepted after review October 6, 2025.
Cite as: Melissa Dzinoreva, Nicole D’Andrea, James Whiteside, Kevin Schulman. 2025. Preventing a Maternity Care Crisis: The Case of Carteret OB-GYN. Health Management, Policy and Innovation (www.HMPI.org). Volume 10, Issue 2.
Introduction
Maternity care deserts are an increasing concern in the United States as access to comprehensive reproductive healthcare continues to decline. According to the March of Dimes 2024 Report, 3,142 counties (35%) are classified as maternity care deserts (Figure 1). These counties lack hospitals or birth centers offering obstetric care and have no obstetric providers, creating a growing public health crisis.[1] Over 2.3 million women of reproductive age reside in U.S. counties classified as maternity care deserts.¹Nearly two-thirds of maternity care deserts are in rural areas, where the average time to access care is 38 minutes, over twice the average travel time (16 minutes) for those in full-access counties.[1] Living in a maternity care desert increases the risk of death during pregnancy and up to year post-partum (aRR for pregnancy-associated mortality=1.91, 95% CI=1.15–3.18; aRR for pregnancy-related mortality=3.37, 95% CI=1.71–6.65).[2] Living in a maternity care desert or low-access county is associated with a 13% and 11% increased risk for preterm birth, respectively, compared to living in a full-access county.[1] Further exacerbating these challenges is the essential role of comprehensive maternity care in breastfeeding initiation, which can improve maternal and infant health outcomes.[3]
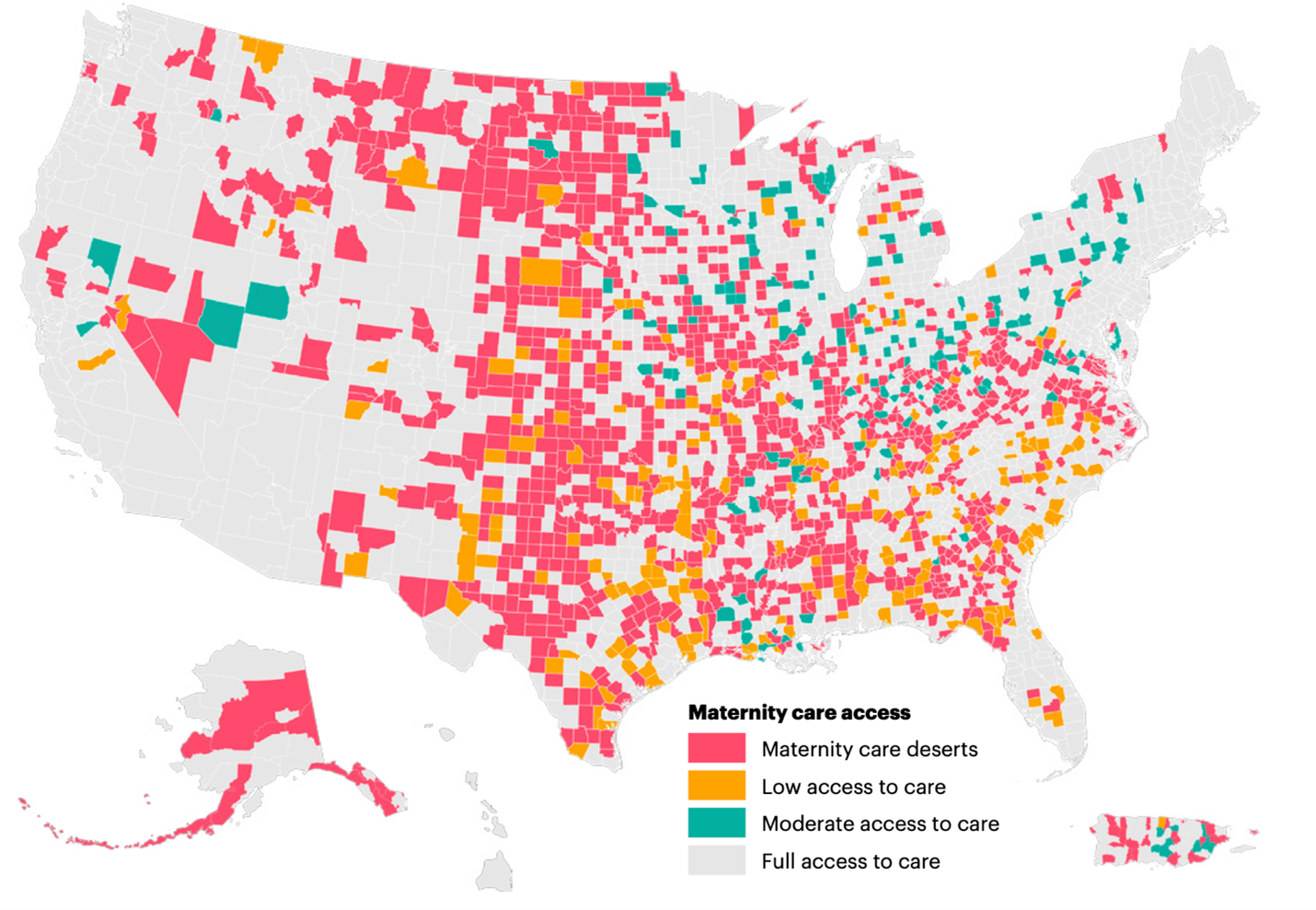
Figure 1. Maternity care access designation by county, US and Puerto Rico1 (Reprinted with permission of The March of Dimes).
While current data provide some information on the extent of this challenge, there are few data informing why a community has lost its obstetric services. We used a case study approach to examine one community at risk of becoming an obstetric desert—Carteret County, NC. North Carolina’s overall maternal health metrics underscore the urgency of this situation. The state ranks 30th in maternal mortality and 39th in infant mortality.[4]
Carteret OB-GYN
Carteret County, located along the eastern coast of North Carolina, has a population of approximately 70,000. The area is renowned for its beaches, including Emerald Isle and the Cape Lookout National Seashore. It also houses marine laboratories for Duke University and the University of North Carolina, underscoring its importance to both the local community and academia. Carteret OB-GYN is the sole obstetric care provider for the county. The six-physician practice operates at Carteret Health Care, a 135-bed independent nonprofit facility. The nearest referral hospital, ECU Health Medical Center, is a two-hour drive away.
Since its establishment in 1977, Carteret OB-GYN has become an integral part of the community. Physicians frequently encounter former patients and the children they delivered, a testament to their longstanding presence in town. The practice was also a leader in the innovative Maternal Outreach Through Telehealth for Rural Sites (MOTHeRS) Project, established in 2020. This initiative was developed in response to gaps in care exacerbated by the COVID-19 pandemic, when many patients missed clinic appointments due to fear and limited information.[5] Women receiving care at Carteret through the MOTHeRS Project reported high satisfaction with the program’s resources, such as food and nutrition education. The practice has maintained the food initiative for patients even after the project’s formal study period ended. Interviews with participants revealed that addressing food insecurity within a clinical setting reduced stress for vulnerable households and lessened the stigma associated with traditional food assistance programs like SNAP and WIC.[6] Carteret OB-GYN believes that their care approach highlights the value of integrating holistic patient support into maternal care.
The Carteret physicians see patients in the office and then take call for deliveries. With six physicians, they average being on-call every 6th night. Vacations are carefully coordinated across the group to minimize the impact on the call schedule. Despite the benefits of practicing in such an intimate fashion with the community, the practice has struggled to recruit new physicians. In fact, at the end of 2024 the most recent member of the group joined six years ago but the rest have been there for between 13 and 27 years. The physicians in the group are realistic about the future of the practice. The oldest member of the group is now 63. Should one physician retire, the remaining physicians are reluctant to do more frequent call. The practice could stop offering obstetric services if they cannot replace the retiring physicians. If that happens, Carteret County could become another maternity care desert. This problem of obstetrician staffing is a common theme across NC labor and delivery units with retirement, practice restriction, and providers leaving all being sources of attrition.
The Rural Obstetrics Practice
Practice restriction has long been a feature of OB-GYN. This cause of obstetrician attrition has accelerated in recent years in part due to professional preferences. CMS funding for graduate medical education (GME) perpetuates a system where most residents train in urban areas with low or stagnant population growth. Since one of the strongest predictors of where residents are employed is where they train[7] physician-density is not commensurate with population growth or need. Further complicating GME training issues, accreditation of OB-GYN residency training programs requires exposure to care that can only be found in more urban areas.[8] Additionally, the demographics of OB-GYN physicians has been cited as a source of practice restriction with a female dominance of physicians entering the specialty[9] More recently, work-life expectations and burn-out have also fueled practice restriction. These factors favor urban practice where there are better employment opportunities for two-career couples, and better access to high-rated schools and cultural attractions.
Commonly medical students applying for OB-GYN residency will say what attracts them to the specialty is the ability to do a little bit of everything. This job characteristic has been both a source of attraction and trouble for the specialty since doing everything meant doing less of any one thing potentially undermining quality. OB-GYN practice is comprised of three “services” – ambulatory, labor and delivery, and gynecologic surgery. This trifurcation is the genesis of sub specialization in OB-GYN. As an untoward effect, specialization reinforces urbanization of care. Subspecialists need a larger captive population to sustain a focused clinical practice. Laborists, while not a formal subspecialty, emerged as a solution to address inpatient obstetrical quality as well as to address labor and delivery staffing.[11] The laborist trend was also fueled by the dramatic shift from self-employment to employment models over the last decade – 55% of physicians now work for hospitals or health systems and 78% are employed in some capacity.[10] All of these restrictions and practice issues have become a “perfect storm” of factors that reducing the availability of OB-GYN physicians outside of urban America. While these issues are far upstream of Carteret County, access to OB-GYN care in the county is an unintended externality of who, how and where OB-GYNs are trained.
Irrespective of its size every community must have a fire department. Similarly, irrespective of how many deliveries a hospital may see there are fixed costs to support the service. Beyond those fixed labor and supply costs, the laborist staff model requires 4.2 full-time equivalents for 24/7 coverage and an attractive call schedule. As these physicians are paid based on compensation benchmarks reflecting urban practice environments, a laborist model is prohibitively expensive for a rural hospital like Carteret Health Care with a modest number of deliveries each month. An employed laborist arrangement also would not address OB-GYN ambulatory or gynecologic surgery care. Hospitals can fill in coverage gaps with locums physicians although these physicians are also expensive and can introduce quality concerns. For an independent hospital seeking to sustain OB-GYN services in a low delivery volume setting, these costs add up to closure of labor and delivery units.
Financial Challenges
Financial instability continues to challenge Carteret OB-GYN, particularly due to its payer mix. From 2014 to 2024, the clinic recorded 7,835 total deliveries. Of these, 3,152 (40%) were covered by commercial payers such as Blue Cross Blue Shield and other private insurers, while the remaining 4,683 (60%) were covered by government sources—including Medicaid, Tricare—and self-pay patients. This heavy reliance on public reimbursement (well above the national average), which typically offers lower payment rates than private insurance, contributes to ongoing financial strain. Essential services such as high-risk prenatal care and mental health support operate at a loss, continued primarily by the dedication of the healthcare staff rather than sustainable funding.
To illustrate the financial challenges further, recent changes to the Medicaid fee schedule in North Carolina highlight the systemic underfunding of obstetric care. As of July 2023, Medicaid reimburses $1,747.98 for obstetric care and vaginal delivery (CPT code 59400), or $697.93 for a vaginal delivery (CPT code 59409) or a cesarean delivery (CPT code 59514) when only delivery services are provided.[12] These rates often fall well below the actual cost of providing the care and do not account for necessary support services, clinic overhead, or the high on-call burden required of rural providers. This structural mismatch between reimbursement and cost contributes directly to Carteret OB-GYN’s financial instability.
Referral Center Perspective
ECU Health Medical Center, the referral hospital for Carteret County that lies two hours away by car, faces significant challenges in assisting Carteret OB-GYN. ECU Health is committed to maintaining its six smaller (less than 500 annual deliveries) labor and delivery units across eastern North Carolina facing similar staffing and financial challenges as Carteret OB-GYN. Over the last five years, ECU Health has documented nearly 25,000 encounters with pregnant women, of whom half had an obesity diagnosis and one in three a hypertensive disorder. Additionally, more than 1 in 10 experienced gestational diabetes while overall one third listed diabetes as a clinical problem. Like elsewhere in the country, the proportion of pregnant women with a chronic medical condition is increasing and placing strain on Greenville’s already understaffed specialists and subspecialists, contributing to longer patient wait times. Greenville-based, ECU Health Medical Center’s capacity issues challenge its ability to manage referrals from Carteret Health Care. Carteret County is not the only county in the ECU Health service area suffering from this rural health care crisis. Given the transportation challenges of poor women living in rural eastern North Carolina, travel to a tertiary medical center beyond Greenville to access care is an unrealistic option for many patients.
The Incoming Tsunami: Workforce and Financial Challenges
The profitability of rural hospital labor and delivery units is not related to low Medicaid or Medicare payments or losses on uninsured patients, but rather to differences in private insurance payments that vary across rural hospitals. Nevertheless, the financial challenges facing Carteret OB-GYN stem largely from inadequate physician funding through the state Medicaid program. While efforts to better compensate obstetric care are essential for sustaining these services, they only address part of the problem. These challenges are exacerbated since, as of October 1, 2025, North Carolina Medicaid has implemented significant reimbursement rate reductions for physicians and other healthcare providers due to a state budget shortfall and insufficient appropriations from the General Assembly.
The deeper, more pressing issue is the workforce. Beyond the issue of specialization, urban training injects another variable into how services are provided to patients in these settings. For example, the explosion of robotic assisted surgery has changed how trainees perform many gynecologic procedures, even when the robotic approach is comparable to the less expensive laparoscopic approach.[13] Since the capital costs of robotic surgery are beyond the means of many rural hospitals, physicians may reject rural practice in favor of working in an urban setting where robotics is available. If GME funding reflected population growth and need, that would be a powerful catalyst for changing some of these biases against rural healthcare. State-level GME funding and loan repayments strategies focused on rural access can also be a source of relief. OB-GYN residency training could prioritize high value care available across all hospital resource settings. Hospital and physician’s payments should similarly incentivize highest value care and not reward the most expensive care. Finally, payments for standby services and low volume adjustments can ease the financial strain experienced by low volume rural labor and delivery units.
After speaking with the dedicated physicians involved, it becomes clear that we are witnessing a crisis slowly unfold. While proposed solutions to address the nations maternity care challenges can focus on adding additional health resources (e.g., doulas), without an obstetrical practice, there is no hospital service. Carteret OB-GYN is under no obligation to maintain its obstetric practice. Meanwhile, the local hospital may soon find itself unable to staff its obstetrics service, either due to the high cost of locum coverage or the complete lack of available providers, potentially forcing the closure of its labor and delivery services. The referral hospital, already challenged by the needs of a high-risk population, is not affiliated with the local hospital and is under no obligation to step in. At the county or state level, there is no designated authority responsible for ensuring the delivery of clinical services.
Watching this crisis unfold, Carteret Hospital and the practice’s ownership group pitched in financially to recruit a new physician to the practice. There was a single candidate who applied, but the practice was able to recruit them and stave off their staffing crisis in the short-term. Other practices in similar circumstances may not be as fortunate.
Conclusion
Carteret OB-GYN’s predicament underscores the broader struggle of rural healthcare systems to balance financial viability with community needs. By implementing targeted policy reforms, increasing financial incentives, and fostering integrated care models, stakeholders may be able to prevent Carteret County from becoming a maternity care desert. However, all of this requires leadership charged with addressing this crisis. Given that nearly 25% of the nation’s population lives in a rural area, access to quality maternal healthcare is a national priority and an investment in the well-being of future generations.
References
- Stoneburner A, Lucas R, Fontenot J, Brigance C, Jones E, DeMaria AL. Nowhere to Go: Maternity Care Deserts Across the US. (Report No 4). March of Dimes. 2024. https://www.marchofdimes.org/. Accessed June 15, 2025.
- Wallace M, Dyer L, Felker-Kantor E, Benno J, Vilda D, Harville E, Theall K. Maternity Care Deserts and Pregnancy-Associated Mortality in Louisiana. Womens Health Issues. 2021 Mar-Apr;31(2):122-129.
- Howell EA, Zeitlin J. Improving hospital quality to reduce disparities in severe maternal morbidity and mortality. Semin Perinatol. 2017;41(5):266-272. doi:10.1053/j.semperi.2017.04.002
- North Carolina Department of Health and Human Services.Maternal and Infant Mortality Statistics Report. 2022.
- United Health Foundation. MOTHeRS Project seeks to improve maternal outcomes in rural North Carolina. UnitedHealthcare Community & State. Published 2020. Accessed May 18, 2025.https://www.uhccommunityandstate.com/content/state-profiles/north-carolina-profile/mothers-project-seeks-to-improve-maternal-outcomes-in-rural-nort
- Saeed SA, et al. Maternal Outreach Through Telehealth for Rural Sites: The MOTHeRS Project.N C Med J. 2023;84(1). https://ncmedicaljournal.com/article/67809-maternal-outreach-through-telehealth-for-rural-sites-the-mothers-project.
- Lee M, Newton H, Smith T, Crawford M, Kepley H, Regenstein M, Chen C. The Benefits of Physician Training Programs for Rural Communities: Lessons Learned from the Teaching Health Center Graduate Medical Education Program. J Health Care Poor Underserved. 2016;27(4A):83-90. d
- https://www.acgme.org/globalassets/pdfs/milestones/obstetricsandgynecologymilestones.pdf. Accessed May 29, 2025.
- Sabbah, G. et al. Bridging the gap: how gender representation in obgyn residency programs compares to other specialties. American Journal of Obstetrics & Gynecology, Volume 226, Issue 3, S1331
- https://www.statista.com/statistics/1479176/share-of-physicians-in-health-systems-us/. Accessed June 1, 2025.
- Tessmer-Tuck JA, Rayburn WF. Roles of Obstetrician-Gynecologist Hospitalists with Changes in the Obstetrician-Gynecologist Workforce and Practice. Obstet Gynecol Clin North Am. 2015 Sep;42(3):447-56.
- https://ncdhhs.servicenowservices.com/fee_schedules. Accessed February 11, 2025.
- Bauer HH, Sahmoud A, Rhodes SP, Sheyn D. Inpatient Hospital Costs and Route of Hysterectomy for Management of Benign Uterine Disease in the 90-Day Global Billing Period. Obstet Gynecol. 2024 Aug 1;144(2):266-274.