Tags: New Research
Brooke Shearon, Kristine Burnaska, and Erin Weber, DataSpring, powered by CAQH; Brooke Istvan, Graduate School of Business, Stanford University; and Kevin Schulman, School of Medicine and Graduate School of Business, Stanford University
Contact: BShearon@dataspring.com
Abstract
What is the message? Payer-provider contracting remains largely manual and document-based, creating inefficiencies and limiting transparency across the healthcare system. Modernizing contracting with standardized, structured, and more digital approaches could reduce administrative burden and better support value-based care.
What is the evidence? Findings are based on data from the 2025 CAQH Index survey, which includes health payers representing 63 percent of covered lives and over 600 provider organizations. DataSpring, powered by CAQH, collaborated with Stanford Medicine to better understand lags in contracting advancements and how the industry can push advancement.
Timeline: Submitted May 4, 2026; accepted after review June 15, 2026.
Cite as: Brooke Shearon, Kristine Burnaska, Erin Weber, Brooke Istvan, Kevin Schulman. 2026. The State of Payer and Provider Contracting: Challenges and Opportunities. Health Management, Policy and Innovation (www.HMPI.org). Volume 11, Issue 2.
Prior Dissemination: This article was published on the DataSpring, powered by CAQH, website on Friday, March 6, 2026. It was promoted on DataSpring, powered by CAQH, LinkedIn, on Monday, April 13, 2026.
Introduction
Contracting between payers and providers quietly shapes how care is financed, how networks are built, and how organizations work together to move healthcare forward.[1] By defining the services providers deliver and how payers reimburse them, contracting ensures patients can access the care they need.[2] Yet new findings from the 2025 CAQH Index [3] show that this critical process still relies on various manual methods. Drawing on the industry’s most comprehensive view of administrative transactions and contracting practices, DataSpring, powered by CAQH, partnered with Stanford Medicine to understand why contracting has not advanced at the same pace as other technological developments in the healthcare industry and what payers, providers, consultants, and policymakers can do to drive modernization.
The 2025 CAQH Index reveals a contracting environment that remains manual, fragmented, and misaligned with the industry’s shift toward more connected, data-driven systems.[4] As other administrative workflows modernize,[3] contracting continues to rely on manual tools and individualized practices that create inconsistency across the industry that drives up costs for all.
These inconsistencies reflect differences in organizational capacity, resources, and priorities, which shape how teams approach contracting and influence an organization’s willingness to change its processes. On the provider side, larger practices often approach contracting with more tools and support, while smaller practices face constraints that limit their ability to change. Payers and providers also prioritize different outcomes, making it harder to move toward shared processes or standardized formats.
This article examines why current variation exists in contracting and possible opportunities for improvement. By addressing fragmented payment arrangements, standardizing contracts, and simplifying payment processes, the industry can begin reducing the billing and insurance-related burden consuming a substantial share of United States healthcare spending without wholesale reform of coverage.[5],[6],[7],[8]
The Document-Driven Approach to Healthcare Contracting
Contracting across payers and providers, particularly agreements governing network participation, reimbursement terms, and associated administrative requirements, continues to rely on manual, document-based workflows that have changed little over time.
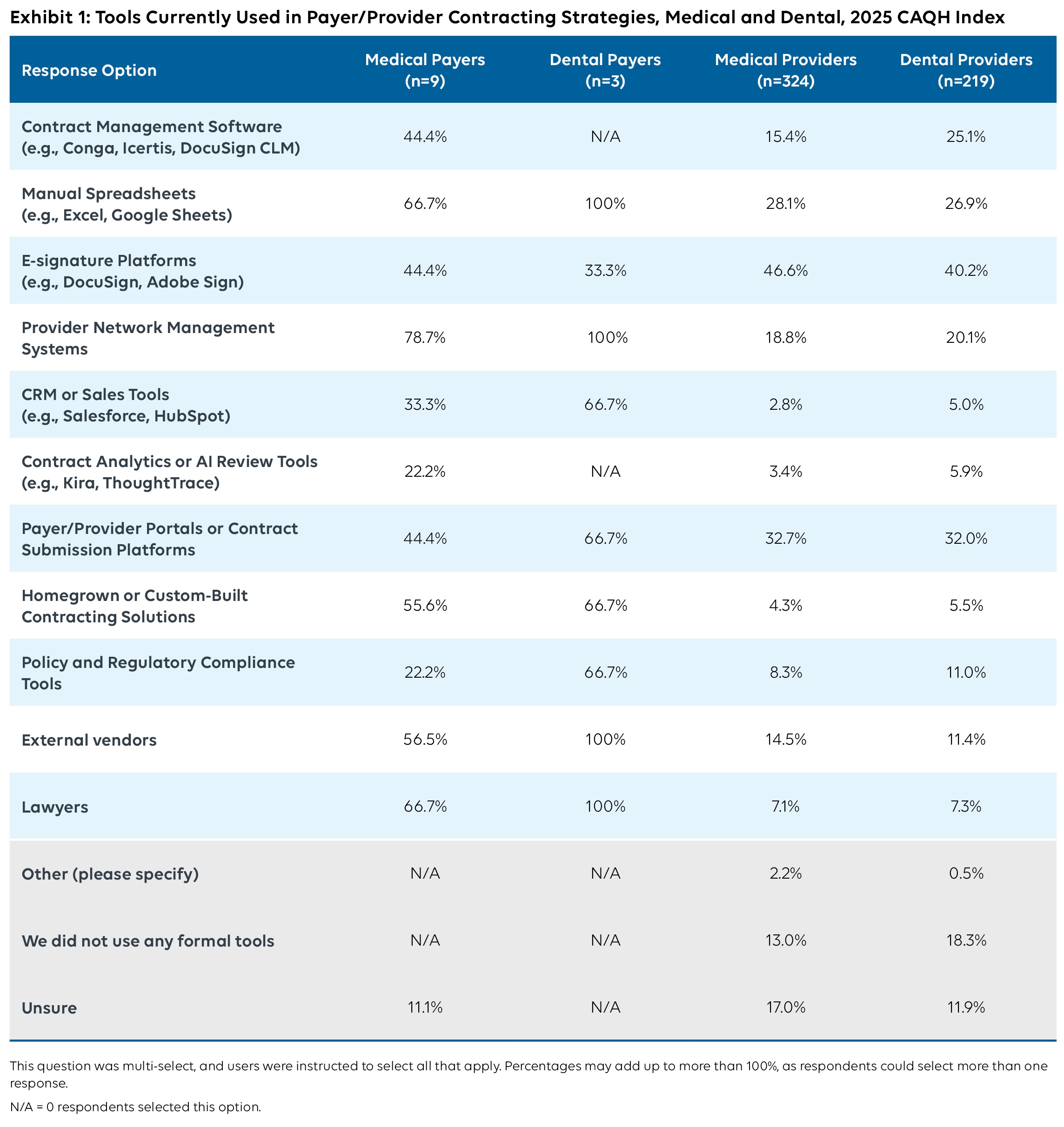
Two-thirds of medical payers and all dental payers report using spreadsheets and lawyers as primary tools for their contracting processes. Providers similarly report use of manual tools, with more than one quarter of medical and dental organizations using spreadsheets for core contracting tasks and more than 30 percent utilizing payer/provider portals.
Reliance on unstructured documents or external relationships makes it challenging to maintain consistent records, understand contract changes over time, or align contract terms with downstream administrative processes. Tools like spreadsheets do not capture reimbursement methodologies or structured regulatory language in ways that support automation, an important factor in reducing operational burden and lowering administrative costs.[9], [10]
Digital tools, such as contract execution through e-signature platforms, are being used to perform specific tasks, with over 40% of medical payers, medical providers, and dental providers reporting use. However, these systems do not transform the underlying content into structured data. Contracts largely remain as PDFs or static files that cannot be easily analyzed or integrated with claims or provider data systems, leaving contracting disconnected from other administrative workflows.[11],[12] Additionally, managing numerous health payer contracts, each with its own platform, format, and timeline, can create a nearly constant stream of administrative work for provider practices.[13], [14]
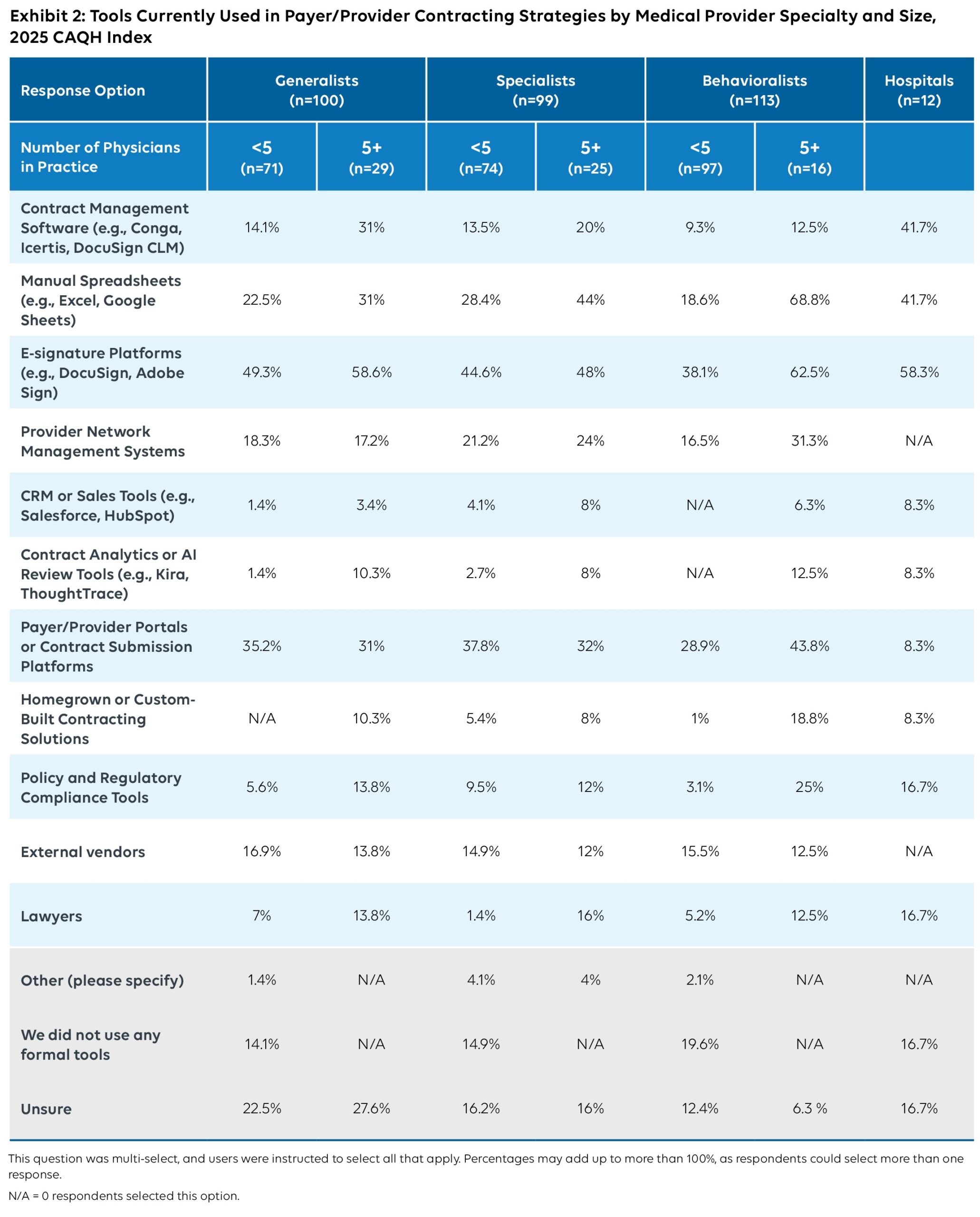
While more advanced solutions, such as provider network management software, contract management software, and contract submission platforms, are available to everyone, they tend to be used by larger organizations with more resources. As shown in Exhibit 2, 42% of hospitals and 31% of large generalists (practices with five or more providers) rely on contract management software compared to 14% of small generalists.
Differences Across Stakeholders and Drivers of Variation
Despite the overarching use of manual tools across the industry, approaches to contracting differ across organizations, shaped by variation in size, staffing, and administrative capacity.
Providers
Larger provider practices tend to approach contracting with more infrastructure behind them. On average, they are about ten percentage points more likely to involve legal review, adopt digital tools such as e-signature platforms, and maintain contract management software than smaller practices across specialties. Larger practices also show higher willingness to adopt new contracting formats (on average, about 14 percentage points more than smaller practices), suggesting that scale and available resources may influence how organizations evaluate potential changes.
Smaller practices operate under different conditions. With fewer administrative resources, they often rely more heavily on external vendor support and portals to manage contracting tasks than larger practices (on average, about three percentage points more). These constraints also affect how they view modernization. Findings show that smaller practices report lower willingness to change their contracting format, particularly if a new approach would introduce additional burden for their teams.
These patterns align with national research indicating that administrative burden falls disproportionately on smaller practices, who often face higher relative administrative costs and have fewer resources to dedicate to modernization efforts.[15], [16], [17] These dynamics make it harder to adopt new systems or participate in standardization efforts. They also contribute to the economic pressures pushing physicians into employed arrangements.[18]
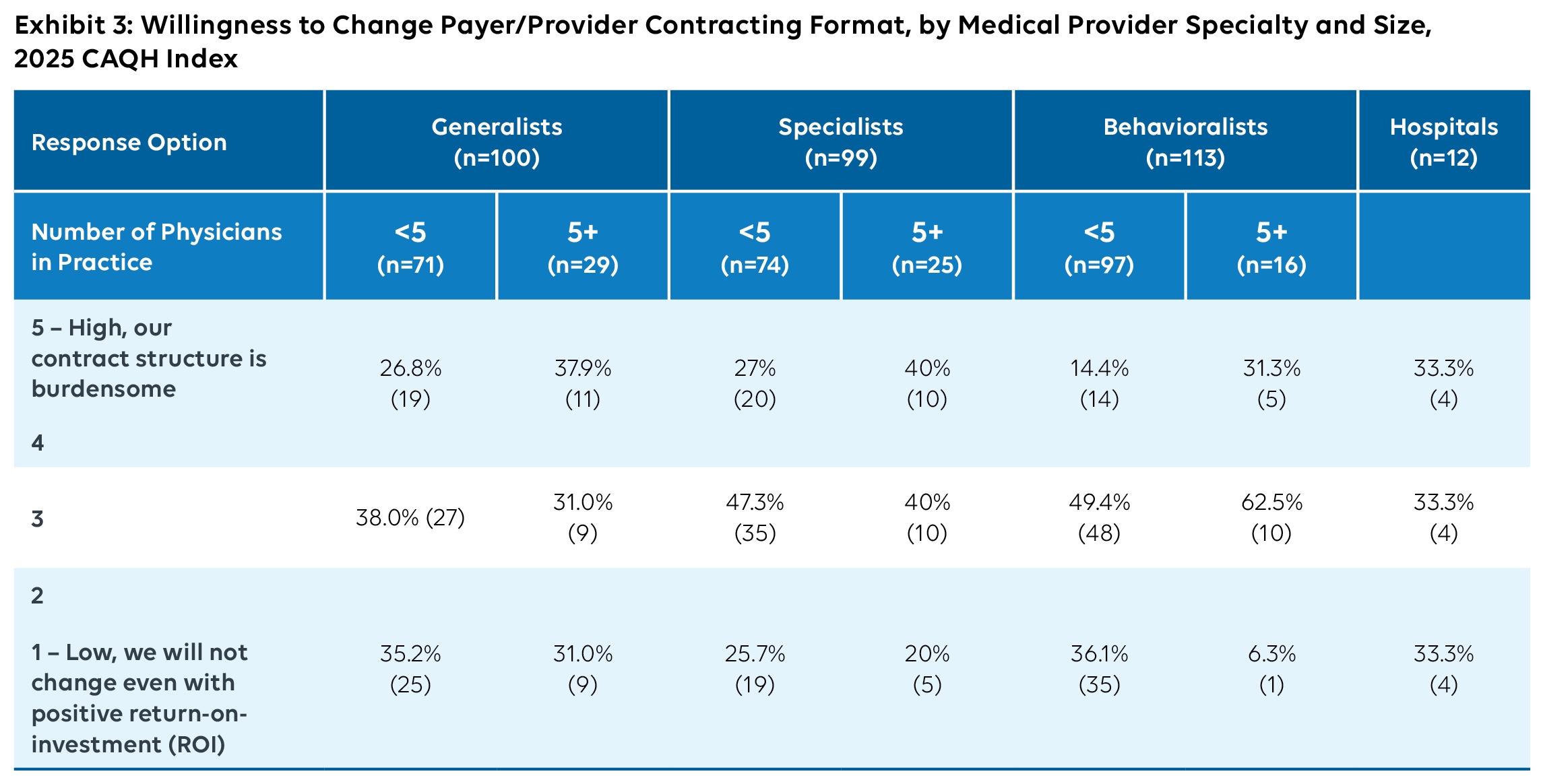
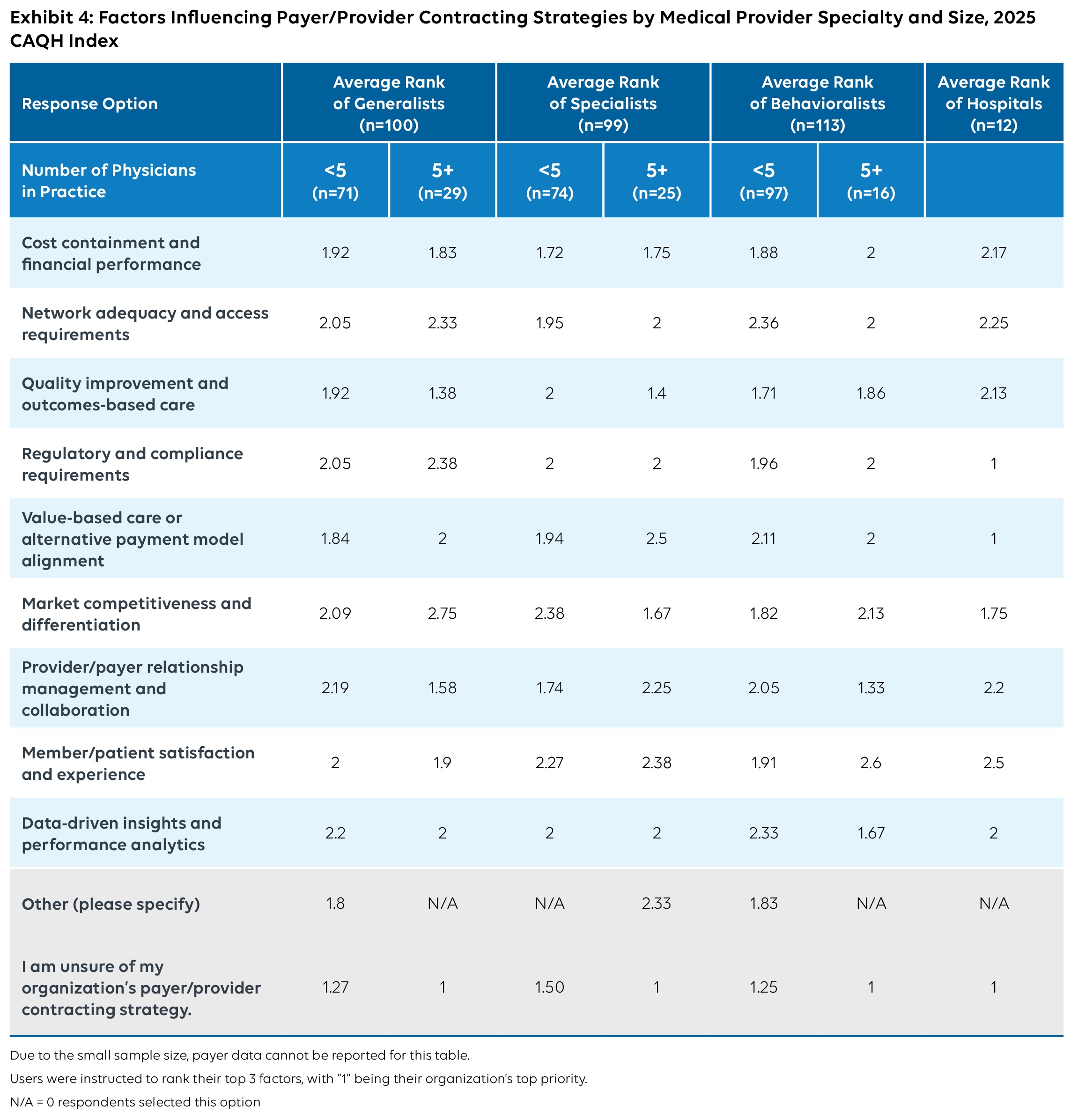
In addition to size, contracting priorities vary by specialty. As shown in Exhibit 4, while hospital-based respondents and generalists cited value-based care or alternative payment models as key influences on their contracting strategies, other specialties placed greater emphasis on quality improvement and outcomes-based care. Additionally, generalists and specialties ranked cost containment and financial performance higher than behavioralists and hospitalists. However, behavioralists and hospitalists were more likely to express interest in changing their organizational or contracting structure, which may indicate that some specialties focus on improving financial performance within existing contracts while others are more inclined to pursue broader structural changes.
These findings indicate that smaller practices need modernization options that reduce net workload without adding additional burden. Larger organizations can use contract management tools to model terms and downstream impacts, but they still depend on payers to simplify reimbursement structures and align contract language with systems.
Payers
Payers approach contracting through a different operational lens, influenced by the scale and complexity of their systems. Most medical and dental payers involve their legal teams throughout the contracting process. More than half of medical payers emphasize maintaining alignment between contracting and operational functions such as claims, payments, and provider data. This reflects the scale and complexity of payer operations but may not align directly with smaller provider needs.[19]
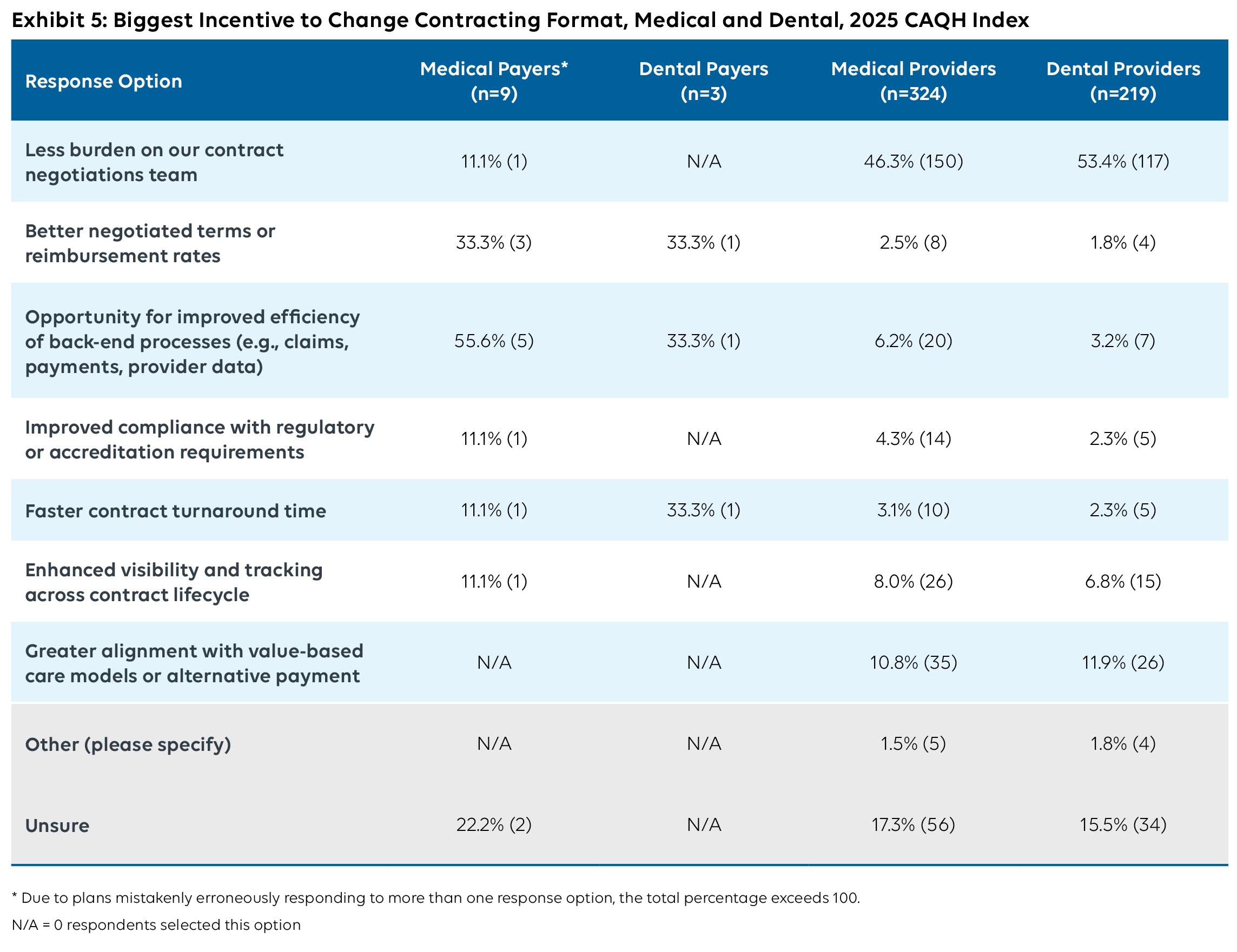
Payers recognize a clear connection between contracting complexity and administrative performance. More than half of medical payers (56%) and one third of dental payers said they would change their contracting format to improve operational efficiency. This highlights a clear opportunity to simplify workflows and reduce administrative burden. Payers are also motivated to pursue contracting changes if those investments lead to better negotiated terms or reimbursement rates (one third of medical and dental payers).
By contrast, medical and dental providers were primarily concerned with reducing the burden on their contract negotiation (46% and 53%, respectively) and showed substantially less interest in negotiated terms (3% of medical providers and 2% of dental providers). Overall, these findings suggest that payers view contracting as a strategic lever to improve both administrative efficiency and financial performance, rather than solely as a transactional process.
Based on the findings, payers recognize the link between contract complexity and administrative performance. To move the industry forward, contracts should be designed as structured, computable data that can flow through claims, provider data, and payment integrity systems over the life of the provider relationship, not just as PDFs.
Lessons Learned and Next Steps
Overall, contracting can become more consistent, predictable, and easier to navigate. Through stakeholder collaboration and element standardization, the industry can align and address underlying sources of variation and reduce administrative burden. Industry workgroups can help define technical guidance to facilitate the use of structured data and workflows. Greater consistency in areas like reimbursement methods, renewal terms, and data-sharing expectations would create a more uniform foundation to work from.[20] Workgroups can also serve as a forum to discuss implementation considerations, including how modernization investments are prioritized and operationalized across stakeholders with varying needs and capabilities. Developing computable contracts could offer a pathway to improved efficiency for health payers and providers across the healthcare system.[21]
To ensure that improvements are effective, efforts should reflect differences across provider types, including primary care, specialty care, and hospital-based organizations. Given the varying contracting needs and capacities across stakeholders, a single, standardized approach may not provide meaningful outcomes, especially for smaller practices. These organizations often face a disproportionate administrative load on already burdened staff, and tools that simplify documents or offer ready-made templates could help modernize the contracting process, making it more feasible. Larger organizations may also benefit from clearer structures, making it easier to align contracting with downstream systems and reducing the time spent reconciling contract terms with operational processes.[22]
For consultants and government agencies, these findings point to a need for end-to-end contracting transformation, not only better rate negotiations. While negotiated outcomes are driven by market dynamics, investments in contracting capabilities can support greater standardization, improved data quality, and more efficient contracting processes. For policymakers in particular, standardizing core contracting elements such as reimbursement methodologies, renewal terms, and data sharing expectations can help advance policy goals related to network adequacy, payment integrity, and provider directory accuracy.
Driving meaningful change requires stakeholders to prioritize modernization efforts, invest in tools and processes that reduce administrative complexity, and collaborate to create a more consistent, data-driven contracting environment. Stronger alignment between payers and providers can reduce administrative steps, increase predictability, and clarify expectations across organizations, regardless of size or stakeholder. By understanding the costs tied to manual processes, organizations can prioritize changes with meaningful impact and become better positioned to support the industry’s shift toward more connected and data-driven systems.[3], [23]
References
[1] American Medical Association. Payor contracting for health care 101 [Internet]. Chicago (IL): American Medical Association; [cited 2026 Mar 6]. Available from: https://edhub.ama-assn.org/steps-forward/video-player/18947118
[2] Medical Group Management Association. Medical practice payer contracting glossary [Internet]. Englewood (CO): MGMA; [cited 2026 Mar 6]. Available from: https://www.mgma.com/payer-contracting-glossary
[3] CAQH. The CAQH Index report [Internet]. Washington (DC): CAQH; [cited 2026 Mar 6]. Available from: https://www.caqh.org/insights/caqh-index-report
[4] Centers for Medicare & Medicaid Services. Application programming interfaces (APIs) and relevant standards and implementation guides (IGs) [Internet]. Baltimore (MD): CMS; [cited 2026 Mar 6]. Available from: https://www.cms.gov/priorities/burden-reduction/overview/interoperability/implementation-guides-and-standards/application-programming-interfaces-apis-and-relevant-standards-and-implementation-guides-igs
[5] Jiwani A, Himmelstein D, Woolhandler S, Kahn JG. Billing and insurance-related administrative costs in United States’ health care: synthesis of micro-costing evidence. BioMed Central (BMC) Health Services Research. 2014;14:556.
[6] Turner A, Miller G, Lowry E. High U.S. health care spending: where is it all going? [Internet]. New York (NY): The Commonwealth Fund; 2023 Oct 4 [cited 2026 Mar 6]. Available from: https://www.commonwealthfund.org/publications/issue-briefs/2023/oct/high-us-health-care-spending-where-is-it-all-going
[7] Scheinker D, Richman BD, Milstein A, Schulman KA. Reducing administrative costs in US health care: assessing single payer and its alternatives. Health Services Research. 2021;56(4):615-625.
[8] Tseng P, Kaplan RS, Richman BD, Shah MA, Schulman KA. Administrative costs associated with physician billing and insurance-related activities at an academic health care system. The Journal of the American Medical Association (JAMA). 2018;319(7):691-697.
[9] Sirion. Understanding healthcare contract compliance: what you need to know [Internet]. London: Sirion; [cited Mar 6]. Available from: https://www.sirion.ai/library/contract-management/healthcare-contract-compliance/
[10] NTRACTS, The hidden causes of spreadsheets in physician contract management [Internet]. Brentwood (TN): NTRACTS; 2025 Nov 12 [cited Mar 6]. Available from: https://www.ntracts.com/blog/the-hidden-costs-of-spreadsheets-in-physician-contract-management/
[11] SolumHealth. Payer contract management: a complete guide for healthcare practices [Internet]. Solum Health; [cited 2026 Mar 6]. Available from: https://www.getsolum.com/glossary/payer-contract-management-guide
[12] Aroris. Understanding the revenue cycle in healthcare: payer contracts [Internet]. Aroris; 2025 Jul 23 [cited 2026 Mar 6]. Available from: https://www.arorishealth.com/blog/revenue-cycle-in-healthcare/
[13] CAQH. The hidden causes of inaccurate provider directories [Internet]. Washington (DC): CAQH; [cited 2026 Mar 16]. Available from: https://www.caqh.org/hubfs/43908627/drupal/explorations/CAQH-hidden-causes-provider-directories-whitepaper.pdf
[14] American Medical Association. 2024 AMA prior authorization physician survey [Internet]. Chicago (IL): American Medical Association; 2025 May 22 [cited 2026 Mar 6]. Available from: https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
[15] O’Malley AS, Gupta DP, Rich RC, Lewis C. Administrative burden in primary care: causes and potential solutions [Internet]. New York (NY): The Commonwealth Fund; 2025 [cited 2026 Mar 6]. Available from: https://www.commonwealthfund.org/publications/issue-briefs/2025/oct/administrative-burden-primary-care-causes-potential-solutions
[16] Scott BA. Reducing regulatory burden – a major opportunity for new administration [Internet]. Chicago (IL): American Medical Association; 2025 May 22 [cited 2026 Mar 6]. Available from: https://www.ama-assn.org/about/leadership/reducing-regulatory-burden-major-opportunity-new-administration
[17] Office of the National Coordinator for Health Information Technology. Strategy on reducing regulatory and administrative burden relating to the use of health IT and EHRs [Internet]. Washington (DC): ONC; [cited 2026 Mar 6]. Available from: https://www.healthit.gov/sites/default/files/page/2020-02/BurdenReport_0.pdf
[18] Physicians Advocacy Institute. PAI-Avalere report on physician employment trends and acquisitions of medical practices: 2019-2023 [Internet]. Chicago (IL): Physicians Advocacy Institute; 2024 Apr [cited 2026 Mar 6]. Available from: https://www.physiciansadvocacyinstitute.org/PAI-Research/PAI-Avalere-Study-on-Physician-Employment-Practice-Ownership-Trends-2019-2023
[19] Douglas C. Navigating the challenges of narrowing provider networks [Internet]. Waterloo (IA): VGM & Associates; 2025 Apr 1 [cited 2026 Mar 6]. Available from: https://www.vgm.com/communities/adapting-to-narrowing-provider-networks/
[20] CAQH CORE. Operating rules [Internet]. Washington (DC): CAQH; [cited 2026 Mar 16]. Available from: https://www.caqh.org/core/operating-rules
[21] Istvan B, Schulman KA, Zenios S. Addressing health care’s administrative cost crisis. The Journal of the American Medical Association (JAMA). 2025;333(9):749-750.
[22] symplr. The real ROI of modernizing contract management in healthcare [Internet]. Houston (TX): symplr; 2025 Dec 3 [cited 2026 Mar 6]. Available from: https://www.symplr.com/blog/contract-management-symplr-value-proposition?
[23] Sahni NR, Gupta P, Peterson M, Cutler DM. Active steps to reduce administrative spending associated with financial transactions in US health care. Health Affairs Scholar. 2023;1(5):qxad053.