Tags: New Research
Becca Nelson, Stanford University School of Medicine, Margaret C Nikolov, Clinical Excellence Research Center, Stanford University School of Medicine, and Kevin Schulman, Stanford University School of Medicine, Clinical Excellence Research Center, Graduate School of Business, Stanford University
Contact: kevin.schulman@stanford.edu
Abstract
What is the message?
What is the evidence?
Timeline: Submitted June 30, 2026; accepted after review June 30, 2026.
Cite as: Becca Nelson, Margaret C Nikolov, Kevin Schulman. 2026. The Growth in Healthcare Administrators since 2004 in the United States. Health Management, Policy and Innovation (www.HMPI.org). Volume 11, Issue 2.
Healthcare administration costs in the United States are the highest of any country,1 yet understanding factors driving these costs remains poorly characterized. One open question is the growth of administrators in the healthcare system.2 Since the passage of the Affordable Care Act (ACA) in 2010, the healthcare delivery system has been transformed by provider consolidation, the migration of physicians to an employment model, consolidation in the health insurance market, and the implementation of myriad value-based payment programs in the public and private sector.3,4
We sought to better characterize the growth of administrators in the U.S. relative to the growth of practicing physicians, and to assess whether the ACA and the subsequent changes to the healthcare market had an impact.
Methods
Data on healthcare administrators was obtained from the U.S. Bureau of Labor Statistics Occupation Employment and Wage Statistics (OEWS) data. Healthcare administrators were defined using the O*NET code 11-9111 for healthcare administrators. O*NET defines healthcare administrators as individuals who “Plan, direct, or coordinate medical and health services in hospitals, clinics, managed care organizations, public health agencies, or similar organizations.” Physicians were defined using all O*NET codes that cover physicians which varied by year over the course of the dataset.
The ratio of healthcare administrators to physicians was computed for each year. Ratios pre-ACA (years 2004-2010) and post-ACA (2011-2024) were compared using one- and two-sample t-tests. Trend over time was assessed using simple linear regression, stratified by period (pre- vs post-ACA). Data analysis was conducted in RStudio v2025.05.1.
Results
The number of healthcare administrators increased from 224,070 in 2004 to 565,840 in 2024 while physicians saw an increase from 471,390 to 778,450 over the same period (Figure 1). Over this period, the ratio of healthcare administrators to physicians increased from 0.48 in 2004 to 0.73 in 2024.
Figure 1: Growth of Healthcare Administrators and Physicians 2004-2024 in the United States.
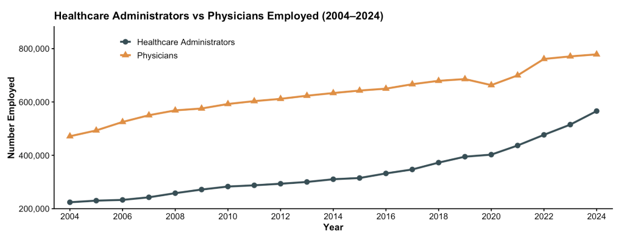
Analysis of U.S .Bureau of Labor Statistics Occupation Employment and Wage Statistics (OEWS) of the number of healthcare administrators and physicians over time. Healthcare administrators grew from 224,070 in 2004 to 565,840 in 2024 while physicians grew from 471,390 to 778,450 in the same period.
In examining changes in the market since the ACA, the mean ratio of healthcare administrators increased significantly from 0.46 (95% CI, 0.45-0.48) pre-ACA to 0.56 (95% CI, 0.51-0.61) post-ACA (p <0.01) (Figure 2). Plotting the ratio of healthcare administrators to physicians over time, the trendline is constant pre-ACA (β̂ = 0.001 [95% CI, -0.01-0.01]), but is increasing over time post-ACA (β̂ = 0.02 [95% CI, 0.02-0.02]). (Figure 2)
Figure 2: Ratio of Healthcare Administrators to Physicians 2004-2024 in the United States.
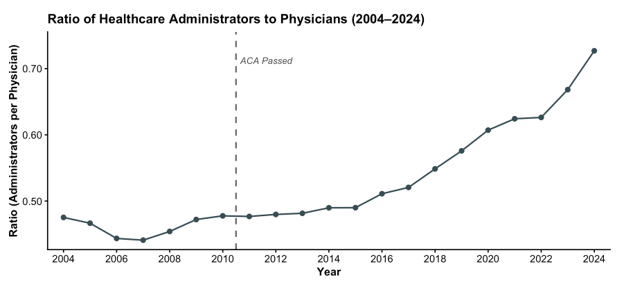
Analysis of US Bureau of Labor Statistics Occupation Employment and Wage Statistics (OEWS) of the ratio of healthcare administrators to physicians over time. The dashed line indicates passage of the Affordable Care Act (2010). The ratio stayed relatively constant around 0.47 until 2011 when the ratio increased regularly until it reached a value of 0.73 in 2024. The trendline for the data points after the ACA from 2011 -2024 is increasing over time whereas there is no difference in the trendline from 0 pre-ACA.
Discussion
The data demonstrate an increase in healthcare administrators both absolutely and as a ratio to physicians, with a significant acceleration of these trends since the passage of the ACA in 2010. (Figure 1,2) The healthcare market has become more complicated over the last decade structurally on the delivery system side, and financially with myriad different payment models, each with distinct prior authorization and data reporting requirements. The result is the growth of non-clinical administrators across the system. Moreover, this growth is continuing (rather than reaching a new plateau). The implementation of technology during this period has not been associated with productivity gains seen elsewhere in the economy.5 Unfortunately, this significant growth in expense and complexity has been associated with a decline in value in the delivery of services to patients.6
Reliable and reproducible data sources for the administrative workforce in healthcare are not readily available.7,8 Data sources providing information about employment of health administrators are imperfect; OEWS data can be recoded frequently and may not include all administrative roles in healthcare systems, but the strength of the data are the survey sample of 1.1 million establishments and detail of 830 occupational categories.
The changes in the healthcare market since the passage of the ACA has led to a significant growth in the number of administrators across the healthcare system, and in the ratio of the number of administrators per physician.
References
- Turner A, Miller G, Lowry E. High US health care spending: where is it all going? Commonwealth Fund. Published October 4, 2023. Accessed February 26, 2026. https://www.commonwealthfund.org/publications/issue-briefs/2023/oct/high-us-health-care-spending-where-is-it-all-going
- Cutler DM. The good and bad news of health care employment. 2018;319(8):758-759. doi:10.1001/jama.2018.1054
- Cooper Z, Gaynor M. Addressing hospital concentration and rising consolidation in the United States. One Percent Steps for Healthcare Reform. Accessed February 26, 2026. https://onepercentsteps.com/policy-briefs/addressing-hospital-concentration-and-rising-consolidation-in-the-united-states/
- Schulman KA. A requiem for value-based care. Health Manag Policy Innov. 2024;9(3).
- Huckman R, Chigurupati A, Cutler D. The IT transformation health care needs. Harvard Business Review. Published November 2017. Accessed February 26, 2026. https://hbr.org/2017/11/the-it-transformation-health-care-needs
- Lescinsky H, Sahu M, Beauchamp M, et al. Exploring state-level change in health care value over three decades in the United States, 1991-2020. Health Serv Res. 2026;61(1):e70054. doi:10.1111/1475-6773.70054
- Brooke Istvan, Heather Bello Thornhill, Karen E Joynt-Maddox, David Cutler, Ezekiel J Emanuel, Availability of consistent, reliable, and actionable public data on US hospital administrative expenses, Health Affairs Scholar, Volume 3, Issue 5, May 2025, qxaf069, https://doi.org/10.1093/haschl/qxaf069.
- Drum K. Join Me On a Dive Down the Rabbit Hole of Health Care Admin Costs. Mother Jones. June 15, 2019. https://www.motherjones.com/kevin-drum/2019/06/join-me-on-a-dive-down-the-rabbit-hole-of-health-care-admin-costs/. Accessed March 5, 2026.