Word from the Editors
On behalf of the editorial team (Regina Herzlinger, Kevin Schulman, Lawrence Van Horn, and myself), I am delighted to welcome you to the current issue of HMPI. We are proud to publish another strong set of articles that help advance HMPI’s vision: We draw from the research and experience of scholars and practicing leaders to provide insights for public and private health sector organizations around the world. This issue kicks off with a set of articles about a question that has huge topical importance: drug prices in the U.S. and elsewhere. This question never lurks far below the surface of political and industry discourse and the current U.S. administration is considering multiple initiatives that would rein in what it believes are excessive prices. The articles in this issue outline the nature of pharmaceutical markets, discuss alternative pricing systems, and consider how moral hazard that arises due to third party payment may contribute to escalating drug prices. The challenge here, of course, is to find a viable balance of cost-effectiveness with continued development of innovative medicines that support health and healthcare in the U.S. and globally. Together, the articles provide a thoughtful base for considering mechanisms that will help find and maintain that balance.
The issue also features strong new research. Karoline Mortensen, Tianyan Hu, Aleeza Vitale, and Hanns Kuttner address the question of whether healthcare providers offer the same services to Medicaid and private patients. Rachel Hadler, Julia Lynch, Julia Berenson, and Lee Fleisher report on a study of how willing patients are to receive services from nurse practitioners rather than physicians, and whether any preference varies by patients’ political affiliations. Gregory Shea, Jeffrey Kaplan, and Stephen Klasko report a study on the impact of leadership development programs for physicians and non-physicians in academic health centers.
We also draw extensively on the experience of thoughtful leaders with an outstanding set of perspectives articles. Mark Simon discusses how obstetrics hospitalists can help reduce perinatal adverse events. Lilac Nachum outlines how the balance between global and local is transforming the scope of opportunities and raising challenges for healthcare professionals and institutions. Steven Ullmann and Richard Westland report on a recent conference that identified issues that are top of mind for leaders in the U.S. healthcare and life sciences sector.
In addition, we are proud to publish the winning entry from BAHM’s 2018 case competition. Elisha Friesema, Stephen Palmquist, and Prachi Bawaskar of the University of Minnesota identify ways of using contagion models from public health to help address the current opioid crisis.
As a final note, we will mention Kristiana Raube’s graduation from the HMPI editorial team. Kristi has taken up the role of country director of the Peace Corps in Liberia. We deeply grateful for Kristi’s leadership in relaunching HMPI. And we are proud of her new leadership in Liberia.
The authors of the articles that we publish in HMPI are committed to improving health systems around the world. We welcome your comments about the articles – please send your comments to us at info@hmpi.org. We also welcome discussion on the BAHM Forum on LinkedIn [https://www.linkedin.com/groups/7042389].
We welcome ideas for potential articles. If you have an idea that you would like to explore for HMPI, please send an outline of your article to our editorial team (info@hmpi.org).
Will Mitchell
Professor of Strategic Management
Anthony S. Fell Chair in New Technologies and Commercialization
Rotman School of Management, University of Toronto
Pharma Prices Are Not Too High (Usually)
Will Mitchell, Anthony S. Fell Chair in New Technologies and Commercialization, Rotman School of Management, University of Toronto
Contact: Will Mitchell, william.mitchell@Rotman.Utoronto.Ca
Abstract
What is the message?
Although drug pricing is highly contentious around the world, with frequent claims of overcharging, average profitability in the pharmaceutical industry is not excessive. Companies need to achieve prices above total average costs if they are to cover the fixed costs of successful and failed development efforts. The most efficient way to accomplish the dual goal of incenting ongoing innovation while also achieving cost effectiveness and broad-based access is to price drugs at different prices in different markets, based on some combination of ability and willingness to pay.
What is the evidence?
Assessment and evaluation of current bio-pharmaceutical industry data, trends, and strategies.
Disclosure: Some of the academic health management programs that I have taught in and several of my research projects have received programmatic support from life sciences companies. This article received no financial or editorial support. All information in the article is based on public sources.
Submitted: October 1, 2018; accepted after review: October 31, 2018.
Cite as: Will Mitchell. 2018. Pharma Prices Are Not Too High (Usually). Health Management Policy and Innovation, Volume 3, Issue 2.
Drug pricing has been controversial in the U.S. and elsewhere essentially as long as drugs have been sold. In 1959-1960, the Kefauver Drug Hearings conducted by the U.S. Senate Subcommittee on Antitrust and Monopoly concluded that pharmaceutical firms did not merit the prices they were charging; [1] moreover, as William Comanor put it in 1966, “the committee charged that little of social value came from industry laboratories”. [2] Scrolling forward to the present, in the past decade or so, prices have escalated far higher, particularly as the biological revolution has taken hold, with some drugs now having list prices in the tens and even hundreds of thousands of dollars.
With increased drug prices has come scrutiny and debate. Perhaps the only thing that the three highest profile candidates in the 2016 U.S. Presidential primaries and election – Donald J. Trump, Hillary Rodham Clinton, and Bernard Sanders – agreed on was that drug prices are far too high. Article after article in the press and media in the U.S. and other countries, as well as highly publicized Congressional hearings, have reported claims of high prices and massive price increases, sometimes targeting individual executives as responsible for price gouging. The current U.S. administration has announced an ongoing sequence of potential initiatives directed at what it believes are excessive prices. [3] And in the 2018 Gallup poll of industry reputation, the pharmaceutical industry finished 29th of 30, with a net negative rating of 23% [30% positive; 53% negative], slightly ahead of only the U.S. federal government. [4] Clearly, drug prices must be too high.
Yet what would it mean for prices to be “too high”? The simplest conceptual case would be that value received by patients and other stakeholders in the healthcare system does not justify the prices charged by pharmaceutical companies and intermediaries such as distributors, presumably because the companies have market power that allows them to price above marginal cost. Yet, as I will argue in this article, a close look at relevant data does not support this conclusion.
Instead, thoughtful assessment suggests that average profits in the pharmaceutical industry are largely in line with the companies’ needs to support ongoing development and commercialization of new drugs and related services. Although some individual cases may be questionable, the overall pattern is one of an industry that typically acts responsibly in supporting necessary business activities while seeking to provide value for patients.
I will start with the assumption that recent advances in drug therapies are making important contributions to healthcare and human health. While there are credible debates about marginal value and concerns about side effects of some drugs and, especially, which patients they might be suited to, there are undoubted major contributions in areas ranging from multiple types of cancer, to Hepatitis C, to a broad set of immunological diseases, to ophthalmic needs, to HIV/AIDS, and a host of other conditions. [5] Moreover, the companies that market these drugs also are increasingly providing a range of support such as infusion services, patient and provider education, patient financial support, nutrition and life style counselling, pay for performance contracts, and other services that provide far more encompassing value than simply a core pill or injection.
Some of these advances of drugs and complementary services serve tens of thousands of people. Others serve only a few individuals who suffer from orphan diseases. Again, while it is entirely reasonable to question whether a particular therapy suits an individual patient in a given context, the overall impact is contributing to solving real human medical needs
Rather than a single price, drugs have multiple prices
Of course, improved health by itself is not enough to end an argument about the industry. There needs to be a corresponding judgement about cost effectiveness [6], as reflected in the price that drug companies receive from the myriad types of payers. This is where the controversy arises. Yet payers, particularly third party payers such as pharmaceutical benefit management companies (PBMs) with substantial market power of their own, have substantial ability to negotiate discounts and rebates, manage formularies, and shape whether drugs achieve market access. [7]
In practice, actual prices to most payers typically are far below list prices that show up in public reports such as Average Wholesale Price (AWP), which one of my colleagues informally likes to refer to as “Ain’t What’s Paid”. Indeed, for almost all drugs, there is no one price – instead, there are multiple prices, sometimes even to the same payer, based on negotiations, public mandates, pressure from patients and patient advocates, and market conditions.
It is not my intent here to argue that any one price to any one payer is “too high” or “too low”. It is the job of any payer to negotiate a price that meets its own definition of value. And there may well be appropriate opportunities to help some payers increase their negotiating strength and sophistication, and so help the healthcare system meet the goals of cost effectiveness and broad access.
Rather, my aim is to argue that the overall revenue that drug companies receive from payers aligns with the health system’s complementary goals of creating incentives for ongoing innovation and for providing as broad access as possible to appropriate health services. Several metrics and practical conditions of the industry underlie this conclusion. In the next sections, I will discuss profitability, the need for average prices of pharmaceuticals to exceed variable costs, and the increasingly short time window for companies to recoup fixed costs of developing and bringing drugs to market before they face generic competition.
Average profitability grew through the early 2000s and then declined
Using companies’ financial statements, I have collected data on more than 70 major pharmaceutical firms that have sold branded pharmaceuticals, including long established companies and new biological entrants based in Western Europe, North America, and Japan, with data for most firms going back into the 1970s or earlier. The most complete period, 1990 to 2017, includes 33 to 50 firms per year, with the numbers varying due to consolidation. Where appropriate, I also draw data on the more than 500 public pharmaceutical and biological firms listed in the Compustat data base. This section and the discussion of costs that follow will be a bit numbers heavy, because it is necessary to use real data to provide an accurate picture of the industry and relevant trends.
The simple story of pharma profitability is that it grew and then declined. In the 1980s and early 1990s, bio-pharma firms’ median profitability based on return on sales (ROS) was about 7% to 11%, a comfortable but not particularly high rate of return. During the 2000s, with the introduction of new generations of large market drugs, median ROS grew to a maximum of 17% in 2009.
Then, between 2010 and 2017, list prices of many high profile new drugs, particularly newly-approved biologicals, increased substantially. One might expect corporate profits to have grown even higher in the past decade.
However, rather than continuing to increase, median return on sales in the industry has declined: falling to 13% to 14% in each year from 2014 to 2017 (the trends are similar if we base profitability on return on assets). Within the average, there is substantial variance. In 2017, for instance, the profitability of 33 companies with a median ROS of 13% ranged from a high of 41% (reflecting gains from the sale of a major business unit) to a low of –9% (reflecting ongoing losses at a biological specialist). In 2016, with median ROS of 14%, the maximum and minimum ranged from 45% (a win from a blockbuster biological) to –56% (the same financially struggling biological specialist as in 2017).
While some firms in some years have achieved particularly high profitability, occasionally even with ROS of 40% or higher – 1.5% of the cases among 1,193 years of observations for 61 unique firms in my data from 1990 to 2017 exceed 40% ROS; 5% exceed 30% – such cases typically last at most for a few years and fall again as competing products enter the market. Hence, even as list prices have increased, average profits in the industry have fallen.
Overall, the bio-pharma industry is now comfortably profitable on average, but far from levels that suggest massive systemic price-gouging. Indeed, major ongoing price reductions on the scale that some critics appear to believe appropriate would quickly lead to untenable financial levels for most or all firms.
Consider the simple math: if the median firm with 13% ROS in 2017 was forced to cut its net prices by 10% with no other changes to its business model, it would barely clear break even. And most of the half of its competitors with ROS below the median value would fall to break even or below. The arithmetic becomes a bit more complicated if the price cut only applied to U.S. sales, which typically mark well over 40% of a U.S. based company’s revenue (and often much higher) and lesser but still substantial proportions for European and Japanese pharma firms, but the financial impact would quickly be unsustainable. Yet a 10% price cut is well below what the debate would suggest is needed.
Cross-industry comparisons of multiple profitability metrics (e.g., return on sales, assets, capital, and equity) based on reports from the industry analyst firm CapitalIQ show that the pharmaceutical and biological industry categories tend to be somewhat more profitable on average than the S&P 500 list of the largest public firms, commonly at about the level of technology and computer hardware companies, but again well within a range of normal profitability. Why, then, have bio-pharma profits declined as list prices – and controversy about prices –have increased?
The costs of doing business have increased
I will highlight four reasons for declining profitability during the past decade: discounts, production costs, R&D expenses, and marketing expenditures. First, part of the cause for the decline in average profitability is the issue I noted earlier: list prices are largely meaningless. During the past decade, third-party payers in the U.S. have become increasingly aggressive about demanding discounts in return for agreeing to include drugs on their formularies of drugs approved for their covered lives. Particularly as competitor products enter a therapeutic class, negotiated discounts commonly increase and net prices fall.
While most discounts are confidential, reports from Kaiser Permanente, investigative journalists, and others suggest that rebates can reach 25% to 50% or more of list price. Hence, while a company with a first-to-market blockbuster may enjoy a few years of high profitability, competition and reactions by payers tend to bring it back down.
Second, many of the newer biological drugs are more expensive to produce than earlier generations of small-cell pharmaceuticals. Median “cost of goods sold” (COGS), i.e., production costs of the drugs, of two dozen major firms I am tracking has grown from about 21% in 2000 to 25% in 2017. While not a huge increase, the extra costs have been enough to affect profits.
Third, the costs of developing and obtaining new drugs have increased due to increasing need for multi-source development activities. It simply is not possible for a single company to possess all the skills needed to bring a full portfolio of drugs to market by relying solely on internal development. Instead, bio-pharma firms now employ a sophisticated set of build, borrow, and buy strategies to source new drugs, including a complex mix of internal R&D, alliances, and acquisitions.
The extent of both acquisitions and alliances has grown strikingly according to figures reported by data bases such as ReCap, Cortellis, CapitalIQ, and SDC Platinum. The annual number of M&A deals has grown from 150 to 200 in the late 1990s, to more than 500 in 2017. Some M&A deal values reach billions of dollars: Cortellis reports more than $250 billion in global bio-pharma acquisition value in each of 2016 and 2017.
Inter-firm alliances in the sector also have become increasingly common. In 1990, fewer than 350 alliances were reported in industry data bases. In 2017, depending on the data source, the reported number had grown to somewhere between 2,500 and 4,000 partnerships. While alliances tend to have lower deal value than acquisitions, annual expenditures now total multiple billions of dollars.
Internal R&D costs, meanwhile, rather than decline as acquisitions and alliances have increased, have also grown. Annual R&D expenditures by 22 major bio-pharma firms in 2000 reached about $32 billion; in 2017, the top 17 bio-pharma companies spent about $73 billion. Across the full set of publically traded bio-pharma firms reported by Compustat, R&D expenditures in 2000 and 2014 grew from $51 billion to $118 billion. In addition to sheer magnitude, R&D has also grown as a percentage of sales: among the leading firms, the average ratio grew from 15% in 2000 to 18% in 2018.
Fourth, selling, general, and administration (SG&A) expenditures also have grown, though at a slower rate than R&D. SG&A is an indicator of marketing and other commercialization activities, including the costs of patient support that are now important parts of the suite of services that complement a core drug. Compustat data for public bio-pharma firms report SG&A growth from about $150 billion in 2000 to $280 billion in 2014.
Despite the growth in magnitude, average SG&A as a percentage of sales has remained stable or even fallen; among the top 30 to 40 firms, the ratio fell from 35% in 2000 to 28% in 2017. The reduction in the marketing cost ratio reflects the shift in strategy during the period, from emphasizing large market drugs such as cardiovascular statins and gastro-intestinal proton pump inhibitors, which require large sales forces, to placing greater emphasis on products such as immuno-oncology drugs prescribed by specialist health care providers, which require more targeted commercial support. At the same time, though, the newer drugs have required substantial patient support as well as market access expenditures in negotiations with third-party payers, which limits the ability to undertake further reductions in expenditure.
The core point here is that multiple aspects of development and commercialization costs have grown more quickly than revenue during the past decade or so, despite the frequent claims of excessive price increases. The expenditures reflect the real costs of doing business in the bio-pharma sector: obtaining and creating new drugs, conducting trials, manufacturing the drugs, gaining market access, and supporting them in the market. Currently, the industry is not under a threat of failure but also is not at any obvious level of excessive profitability that would support extensive price cuts. While individual firms may enjoy very high profits for a few years, they typically return to earth; the overall profile is reasonable. In parallel, firms may suffer low or even negative profits in some years – 14% of the annual observations for the major firms in my data from 1990-2017 report losses – but typically return to reasonable levels, or are purchased by competitors who can use their resources more effectively.
Fixed costs are high, with a substantial gap between variable costs and total average costs
Now let’s leave the deep dive into data and consider the nature of costs in the industry. Bio-pharma is marked by high fixed costs in R&D, whether done internally or paid for via alliances and acquisitions. Successful projects typically require many years and many millions of dollars in lab work, clinical trials, and regulatory expenses, whether initially sourced internally or externally. And many projects fail – that is the very nature of experimentation – sometimes early in the development cycle after a few million dollars but occasionally reaching into the hundreds of millions or more if a drug proceeds to large scale Phase 3 trials before failing.
Figure 1 builds on this point. Development costs, including the costs of failures, are fixed costs. As such, they do not show up in the average variable costs required to produce and support a drug and its associated services in the market. The high relevance of fixed costs creates a substantial gap between “Variable cost to produce” and “Total average cost”, as the horizontal red lines in the figure depict.
Figure 1. Bio-pharma value, costs, and prices
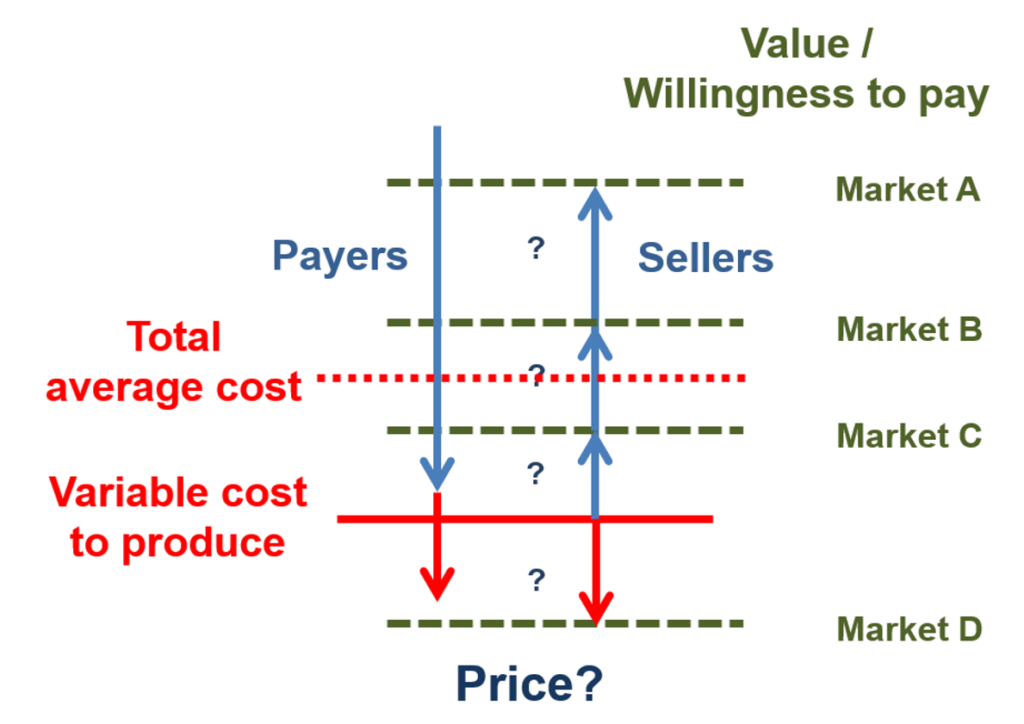
The gap between variable costs and average total costs introduces a major issue in bio-pharma price negotiations. The goal of a pharmaceutical firms’ negotiator is to gain a price as close as possible to a buyer’s value ceiling (the horizontal green dashes in the figure). Yet few buyers will simply pay for the full value they receive from any product – including products that produce health value – if they can negotiate a lower price.
Instead, the goal of any payer is to negotiate price down as close as possible to its estimate of the seller’s average variable cost. That is the minimum price below which a producer cannot cover its operating expenses. And, if pushed to the limit, the variable cost floor is the price that a seller will settle for: this rate at least covers the costs of producing and selling the drug. Where the price ends – up near the value ceiling or down on the variable cost floor – depends on the comparative bargaining power and negotiation skill of the buyer and seller.
This is a challenging negotiating calculus. All payers in the health sector face real pressure on their budgets, with increased prices for pharmaceutical products creating part of those pressures. In the U.S., prescription pharmaceuticals accounted for almost $325 billion in 2015, about 10.1% of national health expenditures (up from 8.8% in 2000), behind the hospital (32%) and physician/clinical (20%) shares. [8] In Canada, drug expenditures reached about 16.2% of national health expenditures in 2016, behind only hospitals (29%), up slightly from 15.4% in 2000. [9] Hence, even though a payer may recognize and even embrace the high health value ceiling of a pharma product, it needs to push as hard as possible to bring prices down toward the variable cost floor.
The individual buyer’s goal to push prices to the floor in turn creates the rub for the seller. If every payer successfully negotiated a price that just met a drug’s average variable cost, then the company producing the drug would fail because it was not covering its fixed costs of development. Instead, a bio-pharma firm requires some degree of negotiating power to charge at least some buyers prices that exceed the minimum market clearing price, shifting up toward the value ceiling.
Indeed, this is one of the purposes of the patent system: to provide a successful innovator with a period of exclusivity in which it can recover the costs of creating the innovation. Then, once a patent ends or, equally powerfully, once a product with similar therapeutic value enters the market, competition will drive prices down toward marginal costs. This balance – of incentive to innovate and competition to bring on subsequent price pressure – is central to patent policy and law.
Now let’s use Figure 1 to make things a bit more complicated, while introducing a necessary part of pharmaceutical pricing strategy. The bio-pharma market, like almost all markets, has multiple segments, with different customers who have differing ability and willingness to pay for a product. In Figure 1, these segments are depicted as Markets A, B, C, and D. For a pharmaceutical company, the goal is to identify the combination of value and ability to pay for each segment and, ideally, settle on prices that come close to that value ceiling for each market, while surpassing variable costs. Such price discrimination strategies are profit maximizing.
Market segmentation introduces pricing variation across and within countries. For instance, prices are commonly lower in lower income countries such as Greece and Spain, versus higher prices in higher income countries such as Germany and the U.S. Even within countries, different payers commonly have different ability to pay. In the U.S., for example, the state-based Medicaid systems are mandated to receive the lowest price negotiated by any other actor, while other payers such as employment-based PBMs commonly have greater latitude and financial resources.
In such cases of multiple market segments with different ability to pay, a pharma company’s dominant strategy is to set different pricing points for each segment. To be sustainable, the strategy needs to result in some prices being high enough above the variable cost floor, in aggregate across the company’s portfolio of products, to cover the gap between that floor and total average costs.
Market D in Figure 1, where buyers are not able or willing to pay enough to cover even the variable costs of production, introduces a further complication. In most industries, sellers would ignore this segment. Yet in healthcare markets, most people – including most people who work in pharmaceutical companies – feel a responsibility to reach as many patients as possible, including those who cannot pay enough to cover operating costs. While no public or private actor can afford infinite below cost contributions, there is real need and desire to provide access to as much of the population as possible. For pharma companies, this is part of the basis of patient assistance programs, which provide subsidized or free drugs and services when people in market D lack insurance or personal resources. In turn, though, such below cost strategies place even more pressure to move well above the variable cost floor when negotiating with buyers in market segments A, B, and C.
Quite simply, “too much” pressure to drive prices down will lead to two negative consequences. In the short term, the pressure will drive out a company’s ability to provide cross-subsidized services below the variable cost floor. In the longer term, the pressure will drive innovative firms out of the market because they cannot cover the gap between variable and total costs.
Time windows before competitors enter have become shorter
Now consider time windows for pharmaceutical companies to earn high prices, even after discounts. The key issue here is penetration of the market by generic drugs and “biosimilars” of biologics. Before the 1984 Hatch-Waxman legislation facilitated entry of generic competitors when drugs came off patent, generic drugs made up about 20% of prescriptions in the U.S. Generic penetration grew to about 40% in 2000. Today, as generic and biosimilar competition has become much more active, and as payers respond to pricing pressure by mandating generics on formularies whenever possible, the generic prescription rate in the U.S. is about 90%. Most traditional developed markets also are at substantial, if somewhat lower, levels; Canada, for instance, has a generic prescription rate of about 70%.
Moreover, under the rules of Hatch-Waxman and similar policies around the world, generic approvals have grown exponentially. In 1984, the U.S. FDA reported 66 approvals; in 2017, there were 847 generic approvals. [10] Generic competitors are commonly lined up to enter the market immediately when a drug goes off patent, particularly if the drug had achieved a substantial market size.
Once generic competitors enter, prices fall, sometimes drastically. Prices for traditional large market drugs with multiple generic competitors commonly face price reductions of as much as 90%. Price reductions for the specialized biologicals that have begun to go off patent and face biosimilar competition have been less striking, because so far there are fewer competitors. Nonetheless, the reductions are substantial, with discounting in the range of 35% commonly being reported.
Once generic competition becomes active, prices move, often rapidly, toward the variable cost floor in Figure 1. From the point of view of payers, this is a good outcome. And, again, this is one of the goals of the patent system: provide a period of exclusivity as an incentive to innovate, then open the doors to competition to create incentives to innovate again as well as providing cost effectiveness in the market.
From the point of view of a bio-pharma innovator, though, this increasingly striking combination of early generic entry and strong price reductions means that there are far fewer years than there once were to earn the profits needed to cover the gap between variable and fixed costs. If the firm is going to survive, it needs active strategies to deal with the shorter window.
Time window strategies have had two major components, both of which we have noted earlier. First, companies are increasingly emphasizing specialty drugs. This is partly a feature of the biological revolution, which has created opportunities for major contributions to health for targeted medical needs. In addition, drugs for specialty market segments such as oncology and immunology, whether based on biological or older science, typically face lower rates of post-patent generic competition, both because only a few firms currently have the skills needed to compete effectively and because specialty prescribers and patients are often reluctant to switch away from drugs that they have come to understand and rely on. Hence, even after patents expire, specialty drugs commonly achieve prices above the variable cost floor, sometimes for multiple years.
Second, firms have increased the initial prices they charge during the shorter protected window, in order to generate income as quickly as possible before facing generic or biosimilar competition. Thus, the policy changes that have encouraged price competition from generics – as desirable as these policies undoubtedly are for payers, patients, and the health system – have also created strong pressures to increase prices that policy makers are now complaining about. The quid of competition and long term price reductions has induced a pro quo of initial price increases.
Where does this leave us?
The key question is whether healthcare systems in countries such as the U.S. are now reasonably close to achieving a balance of innovation and cost effectiveness or, as some voices implicitly claim, can we continue to maintain incentives to innovate while drastically bringing down pre-generic prices? My interpretation of the data and observation of strategies and incentives is that we are fortunate to have an actively innovative bio-pharma sector, made up of a complex and dynamic mix of established firms, new ventures, academic and government scientists, complementary firms, and regulatory bodies, paralleled by a critically important set of generic manufacturers (some of which are the same companies) that help provide discipline in the system. This quasi-market is far from fully efficient – no market is – but it has evolved to a point of generating and commercializing new bio-pharmaceutical products and supporting services at a rate that is higher than at any point in the history of the industry.
Consider recent innovation. Just as approval of generics is increasing, so is approval of new drugs. In 2017, the U.S. FDA reported granting 54 new approvals, including 21 biologicals. This was the highest rate ever (other than a 1996 clean out of the approval pipeline), up from 29 (2 biologicals) in 2000. The companies that received the approvals included a wide mix of established pharmaceutical firms from Western Europe, Japan, and the U.S., plus an even wider mix of new ventures and smaller specialty companies.
Now consider market entry. Innovator companies commonly apply for FDA approval and introduce their drugs to the U.S. market before entering other countries. The prices available in the U.S. are not as much higher than those in other traditional developed markets as reported list prices would suggest, but on average are somewhat higher, due in large part to the multiple segments available for price discrimination. In turn, profitability in the U.S. is higher: the few firms that report geographic profit margins commonly recognize operating profits as a percentage of sales that are 15% to 25% higher in the U.S than in Europe. Higher prices and profits typically lead to faster entry, earlier access to novel treatments, and ultimately, earlier access to lower-priced generics once the innovators’ patents expire.
It is important to recognize that there are outliers in the system. Some companies earn very high profits, though typically for only a few years. In part, the hope of such profits can be viewed as a lottery that incents entry to the industry. Indeed, there are far more companies with very negative profitability than very positive results – the median return on sales of all bio-pharma companies in the Compustat data base (now more than 500 firms) has been negative each year since 1989. The lure of a payoff is a necessary complement to the uncertainties of experimentation.
There are also outliers in pricing strategy that on the face, and likely even the depths, of it do appear unreasonable. Massive increases in prices of sole-source generic drugs that can be maintained until competitors gain approval and enter, which typically takes several years, stick in many craws. But it is important to recognize that these are outliers and not to develop general policies targeted at extreme cases.
A key point here is that it is equally important to recognize that lower prices typically lead to later entry and sometimes no entry at all. Introduction rates to lower priced southern European markets, for instance, are substantially lower than in North America or much of northern Europe. Simply forcing prices to a lower level in any given country, whether the U.S. or elsewhere, would almost certainly lead to reduced entry in that country.
Nonetheless, there is an active policy and health question here, of when higher initial prices in a market – and consequent more active entry – are balanced by greater health benefits. The answer to that question requires engagement of multiple stakeholders in the health system, including payers, prescribers, regulators, bio-pharma companies, and patients. Currently, once a drug has received market approval, payers such as PBMs have become increasingly powerful gate keepers in access, with their role in setting formularies. There is real strength in that role, but there are also opportunities for more effective engagement of the other stakeholders in assessing costs and benefits.
If there is a need for policy initiatives, the goal of integrating insights across the fragmented silos of the healthcare system in the U.S. and elsewhere is far more of a priority than the marginal reductions in prices that could be accomplished without drastically damaging the ability of innovator companies and their generic followers to provide continuing health value. Rather than the current debate about costs, we would be much better served by a debate – and action – about appropriate value.
References
- Daniel C. Morgan, and Samuel E. Allison. 1964. The Kefauver Drug Hearings in Perspective. Southwestern Social Science Quarterly, 45 (1): pp. 59-68. https://news.gallup.com/poll/12748/business-industry-sector-ratings.aspx
- William S. Comanor. 1966. The Drug Industry and Medical Research: The Economics of the Kefauver Committee Investigations, The Journal of Business, 39 (1): pp. 12-18. https://www.jstor.org/stable/2352011?seq=3#metadata_info_tab_contents
- Yasmeen Abutaleb and Michael Erman. 2018. Trump seeks to base Medicare drug prices on lower overseas rates. Health News, October 25. https://www.reuters.com/article/us-usa-trump-drugpricing/trump-seeks-to-base-medicare-drug-prices-on-lower-overseas-rates-idUSKCN1MZ2SF
- https://news.gallup.com/poll/12748/business-industry-sector-ratings.aspx
- As one of many examples of studies of health benefits, see a discussion of health benefits for rheumatoid arthritis see: John J. Cush and Kathryn H. Dao. 2007. Perspectives on Safety vs. Benefits of Biologic Therapies. Medscape Rheumatology. https://www.medscape.org/viewarticle/553515_4
- Robert S. Kaplan, Michael E. Porter, Mark L. Frigo. 2017. Managing Healthcare Costs and Value. Strategic Finance 98 (no. 7): pp. 24–33.
- Cole Werble. 2017. “Health Policy Brief: Pharmacy Benefit Managers,” Health Affairs, September 14, 2017. DOI: 10.1377/hpb20170914.000178
- Centers for Medicare & Medicaid Services, Office of the Actuary, National Health Statistics Group.
- Canadian Institute for Health Information (CIHI): https://apps.cihi.ca/mstrapp/asp/Main.aspx
- Drugs@FDA: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Reports.NewOriginal_ANDA
Healthcare Leaders Reflect on the Business of Healthcare Today
Steven G. Ullmann, PhD and Richard Westlund, MBA, University of Miami Business School
Contact: Steven G. Ullmann, sullmann@bus.miami.edu
Abstract
What is the message?
What issues are top of mind for leaders in the U.S. healthcare and life sciences sector
What is the evidence?
Discussion among industry, clinical, and policy leaders at the University of Miami’s annual “Business of Health Care” conference on topics ranging from healthcare policy to the opioid epidemic.
Submitted: May 18, 2018; accepted after review: July 20, 2018.
Cite as: Steven G. Ullmann, Richard Westlund. 2018. Reflections by Health Care Leaders on the Business of Health Care. Health Management Policy and Innovation, Volume 3, Issue 2.
The Center for Health Management and Policy at the Miami Business School, University of Miami, recently hosted our seventh annual conference on “The Business of Health Care.” Our objective at each conference is to understand how the different sectors of the health care industry are impacted by changes in government policies, as well as technology, finance, and consumer trends. Most generally, we want to understand how the health care sector is impacting business and society as a whole.
This year’s conference theme, “What’s Next?”, drew more than 700 business executives, health care professionals, and students, including regional, national, and global leaders in their fields. The focus was on how the failed Congressional effort to repeal and replace the Affordable Care Act (ACA) would affect the health care sector, heathcare access, cost, and quality, as well as business in general.
This year’s panel consisted of Pamela Cipriano, President of the American Nurses Association; Joseph Fifer, President and CEO of the Healthcare Financial Management Association; Richard Pollack, President and CEO of the American Hospital Association; Marilyn Tavenner, President and CEO of America’s Health Insurance Plans; and Halee Fisher-Wright, M.D., President and CEO of the Medical Group Management Association. The panel was moderated by Patrick Geraghty, CEO of GuideWell Mutual Holding Company, the parent company of Florida Blue.
Discussion initially focused on healthcare policy developments in Washington, D.C. The consensus was that with the midterm elections looming, little legislative action was expected from Congress. Rather, there have been policy changes from the executive branch through adjustments to regulations and tweaks to the Medicaid system. Two key areas of change were federal approval for health plans that are not totally compliant with the Affordable Care Act, and the movement away from national policy to state policy with respect to Medicaid access and coverage.
Access to private insurance was another point of discussion. High premiums, copays, and deductibles are impacting and implicitly challenging the concept of healthcare as a right in the United States. To address limitations in access to healthcare, the panelists discussed allowing nurses to practice at the highest levels of their education and training. While licensing policies differ from state to state, this could help address the access issue, both financially and geographically.
There was significant discussion concerning the value proposition:
Value= Quality/Cost,
and the movement from volume- to value-based reimbursement. Hospitals are seeing the move from fee-for-service to fee-for-value. Value is being addressed with focus on such aspects as readmissions, non-compliance with reform experiments, and shared-risk CMS programs for physician practices and other provider organizations. However, population management and capitation methodologies are still not widespread. The panelists also examined the many pilot projects associated with the creation of value, such as the 80 payment reform experiments underway in one large healthcare system alone. Further, the Accountable Care Organization trend has had mixed success, although it may be helping to bring some care teams into alignment.
One of the items on panelists’ minds was the opioid epidemic in the United States. It was indicated that the nursing profession is on the front line of pain management. There have been in excess of 50 bills discussed in Congress (though that has narrowed down to one). At the same time that there has been a crackdown on prescription opioids. Indeed panelists indicated that, because of the attention paid to the issue, that there has been a 30-40 percent drop in opioid prescriptions.
It was made clear, however, that there is a role for opioids in the management of pain in both the hospital and home care environments. Unfortunately, now we are in a situation where those who prescribe opioids are “being blamed.” The panelists also noted that while much attention has been paid to the opioid epidemic, issues associated with alcoholism and alcohol-related deaths have not been discussed in depth, although they are also a very serious public health issue.
Returning to the theme of value-based purchasing (Quality/Cost), the panelists quickly came to agreement that an area of significant opportunity was in the management of chronic conditions. Given the aging of Americans, a focus on wellness, patient compliance, care at home, and human contact can all significantly improve quality of life without adding significantly to the cost side of the equation. This is an area where Congress is in need of education as to effective spending especially given the limited federal budget to attain the most effective patient and population health outcomes.
Reflecting the diversity of the panelists – who represented medical group management, nursing, hospital and health care systems, financing of these systems, and providers, as well as the insurance sector – the closing remarks centered on the need for teamwork to improve the quality of medical care and patient outcomes in the U.S. and globally in a cost-effective manner.
First Do No Harm: How an OB Emergency Department Can Help Reduce Perinatal Adverse Events
Mark N. Simon, MD, MMM, CPE, Ob Hospitalist Group
Abstract
What is the message?
Obstetrics is a highly-charged environment. Under the traditional “call model” of hospital obstetrics, siloed care can create an atmosphere ripe for error. Hospitals can reduce adverse events by identifying the factors that lead to gaps in care and implementing better solutions. An examination of claim frequency data suggests an OB hospitalist program centered on early team-based involvement and assessment of the patient is associated with reducing harm from occurring during labor and delivery.
What is the evidence?
Data from Clarity PSO reveals that the second highest rate of harm events (among event types) are perinatal events, with 66 percent involving harm, compared to 24 percent of “no harm.” An analysis by Ascension Health of key risk mitigation strategies identified the use of OB hospitalists at their hospitals as a valuable best practice initiative in driving down the loss, with a 31 percent reduction in serious harm incidents before and after program implementation.
Submitted: July 11, 2018. Accepted after review: July 20, 2018
Cite as: Mark N. Simon. 2018. First Do No Harm: An OB Emergency Department Can Help Reduce Perinatal Adverse Events. Health Management Policy and Innovation, Volume 3, Issue 2.
“Adverse event” is an oddly innocuous and impersonal word when used in context of healthcare delivery.
Technically, “adverse event” describes a clinical incident where unexpected injury/harm is caused by medical management or a complication rather than the underlying disease. But the term “adverse event” removes the incident from its genesis – the root cause of harm – and harm is personal and rarely innocuous.
For the patient, an adverse event can impact safety, health, and well-being, often leaving in its wake anger, sadness, pain, and grief. To a clinician, an adverse event means something, be it major or minor, went wrong with his/her patient care; the thought of possibly playing a role in that error can lead to self-blame, doubt in professional abilities, depression, and burnout. And even a community also bears some of the impact of an adverse even, albeit in a less personal way. Healthcare may be a business, but it also is a service delivered by individuals and respected community institutions. When an adverse event occurs, there is risk that the community will lose trust in a clinician or a beloved institution.
Adverse events also have wide-ranging ramifications and a long shelf-life. For hospital administrators, risk managers, or c-suite executives, an adverse event can make it challenging or impossible to achieve organizational goals, and more likely lead to impacts ranging from reputation damage to exposure and litigation.
Now, add to that powder keg the unique dynamics of a hospital obstetrical unit.
There is the hope and possibility, but not the guarantee, of a happy, healthy outcome for mother and child. This is not only the outcome that is desired by the family, but also an outcome that is assumed by modern society. So when an adverse event occurs, the ripples and repercussions are even more pronounced.
Given these dynamics, there is enhanced potential for processes to break down and rapid response times to lengthen. By its very nature, the unexpected can occur in this setting, and an uneventful delivery can quickly become a life-threatening emergency. In comparison to other medical professions, obstetrics is also anomalous in that not just one life is at stake, but two.
In a perfect world, adverse events would not occur in obstetrics. But healthcare is imperfect; despite best practices, we don’t have the ability to preempt emergencies, the tools to change or reverse the inevitability of disease progression, or the answer to every medical mystery. On top of that, healthcare – like a baby – is delivered by humans. And humans make mistakes.
What if we focused on transforming the Labor & Delivery structure so that mistakes rarely occur?
While adverse events may never be totally eliminated, we can pursue that goal by not just tracking, but by better understanding the data related to adverse events, addressing the factors that lead to gaps in care, and filling those gaps with better systems and solutions. In short: in addition to lowering harm events themselves through obstetrical best practices, we must avoid potential for harm by changing the ecosystem itself.
Healthcare delivery systems can start that process by closely examining Patient Safety Organization (PSO) perinatal practice data to identify opportunities for interventions. In general, “harm events” can be characterized as having no harm (in that a reportable event happened but there was no harm done); mild harm; moderate harm; severe harm; or death. Many hospitals examine their data and classify their events into one of those five categories.
A recent examination of data on harmful events by Clarity PSO, one of the nation’s largest Patient Safety Organizations, reveals that the second highest rate of harm events, within event types, are perinatal events. Given the reasons outlined above, perhaps that is to be expected. But of those, 66% involve harm, compared to 24% of “no harm.” In almost every other category, “no harm” events are about twice as high as “harm events.”
These data suggest that, even in highest risk area of medicine, harm reduction initiatives may not go far enough in getting to the fundamental cause of adverse events. But the data also speak to complexity of OB/GYN care – and the importance of having a team-based approach to collaborate proactively, and to anticipate potential problems that could result in unintended harm.
In a traditional call model, there are numerous factors that may contribute to an environment ripe for error. Those factors include disparity of care, reliance on telephone triage, delays in care, patient miscommunication/dissatisfaction, doctor/midwife practice interruptions, and doctor/midwife stress and fatigue. Many of these factors are exacerbated by the siloed care that occurs in the traditional call model, in which one nurse runs triage for a presenting patient and then communicates, often without the benefit of the full clinical picture, to other stakeholders including the clinician. Both individually and collectively, these factors detract from a culture of safety and harm reduction.
Worse, the traditional call model is based on the “wait….wait…wait…NOW!” system of delivery. Under the watchful eyes of the nursing staff, a woman labors until the decision is made to call her obstetrical clinician, at which point the OB must drop everything – seeing patients in her clinic, having dinner, sleeping – and get to the hospital for the delivery. That potential delay in care is associated with 31 percent of OB claims (22% related to delay in recognizing and treating fetal distress, another 9% with delays in delivery).[1]
The laborist model, in theory, was designed to surmount those challenges. A term first coined in 2003, “laborists” were OB/GYNS who were primarily responsible for the management of laboring women and emergencies in Labor & Delivery. As the model evolved – and terminology changed to “ob/gyn hospitalist” – the American College of Obstetricians and Gynecologists added its stamp of approval, noting in a Committee Opinion that it, “…supports the continued development and study of the obstetric and gynecologic (OB-GYN) hospitalist model as one potential approach to improve patient safety and professional satisfaction across delivery settings. Standardization of medical care has been shown to lead to improved outcomes, and OB-GYN hospitalists can serve as a driving force behind the implementation of these protocols in labor units.”[2]
Since 2003, hospitals have explored differing models with varying degrees of success. Some hospitals use in an in-house model, in which existing staff OBs perform limited OB/GYN hospitalist duties. This can be difficult for these clinicians who are simultaneously caring for their private patients while performing OB/GYN hospitalist duties, making them susceptible to being over-extended. Other hospitals use a physician employment model, in which physicians who may or may not also have a private practice are employed by the hospital to perform a contractual list of OB/GYN hospitalist duties. A third option is the management model, in which hospitals contract with outside companies to recruit and manage OB/GYN hospitalists who provide a wide array of services, implement the program, and oversee its operation.
An aspect included in some of these models that has emerged in recent years is the Obstetrical Emergency Department (OBED). Under an OBED model, all OB patients presenting with an emergency condition are seen by a physician or midwife alongside the obstetrical nurse. Emergent issues are quickly addressed by an OB/GYN with specialized training in those situations. For patients without a primary obstetrician at the hospital, the OB hospitalist cares for the patient from arrival through discharge. For patients whose obstetrician practices at the hospital, the OB Hospitalist addresses the emergent situation with which the patient presents and then coordinates continuing care with her primary obstetrical clinician.
The nucleus of this model is that the nurse and hospitalist work together to triage and take a team- based, “first touch” approach to presenting patients in the OBED. This ensures that the patient begins on a care path that has more effective communication, timely intervention, and proactive identification of potential issues. It helps to eliminate the silos that can lead to harms in care.
A recent study conducted with Ascension Health, the largest non-profit health system in the U.S., offers empirical evidence that this “first touch” model may provide significant benefit in reduction of serious harm incidents. The case study examined the key risk mitigation strategies that resulted in favorable loss trends / claim reduction for the organization in recent years; the researchers supported their analysis with Willis Towers Watson’s National OB benchmarking study of >550 birthing hospitals.
The analysis found that the health system experienced lower claim frequency, and lost cost per birth, than average industry trends found in the benchmarking study, and identified the use of OB hospitalists at their hospitals as a valuable best practice initiative in driving down the loss. Specifically, the analysis identified a 31 percent reduction in serious harm incidents before and after implementation of OBED programs.
A deeper look at PSO and the Ascension data suggests that this “first touch” OBED approach reduces harms because it is structured to lower the potential for harm. Under the OBED model, most patient encounters in Labor & Delivery begin with assessment and triage by an OB/GYN hospitalist. Even if an OB hospitalist is not involved in the delivery, or ultimate co-management of patient, the harm data suggests that it is the early team-based involvement and assessment of the patient that is critical in reducing harm from occurring during their labor and delivery.
A 2015 study by researchers at Northwestern University found adverse events or potential adverse events occurred in approximately 1 in 5 women admitted to a labor and delivery unit.[3] Up until the last few decades, mitigation has focused on improving the practice of medicine – a critically important effort, but one that PSO data tells us must be coupled with transformation of the Labor & Delivery environment. The World Health Organization’s 2012 Every Woman, Every Child (EWEC) Innovation Working Group (IWG) report notes that, “Much of healthcare and health-systems based research has focused on pioneering new science. More recently there has been a focus on services already in place — specifically, investigating how to minimize harm in existing health systems and understanding better how current healthcare practice can be made to be as effective and efficient as possible.”
It would be welcome irony if the impersonal “adverse event” was eliminated by focusing on the most personal aspect of the delivery of perinatal care: a clinical “first touch.”
References
- The Doctor Company, 2007-2013 Malpractice Claims
- https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Patient-Safety-and-Quality-Improvement/The-Obstetric-and-Gynecologic-Hospitalist
- The frequency of and factors associated with adverse events on labor & delivery Chadha, Angad et al. American Journal of Obstetrics & Gynecology , Volume 212 , Issue 1 , S63
Healthcare – An Industry Unlike Any Other Goes Global
Lilac Nachum, PhD, City University New York, Baruch College [1]
Contact: lilac.nachum@baruch.cuny.edu
Abstract
What is the message?
How the balance between the global and the local is transforming the scope of opportunities and raising challenges for healthcare professionals and institutions.
What is the evidence?
This paper is derived from a course on the globalization of healthcare developed and taught by Professor Nachum as part of Baruch College MBA program for Healthcare professionals. It is based on a variety of secondary sources and was informed by class discussions with the healthcare professionals enrolled in the course
Submitted: March 19, 2018; accepted after review: June 15, 2018
Cite as: Lilac Nachum. 2018. Healthcare: An Industry Unlike Any Other Goes Global. Health Management Policy and Innovation, Volume 3, Issue 2.
The Globalization of Healthcare
The healthcare industry[2] has been transformed in recent years from what was traditionally a primarily domestic industry into an increasingly global industry, defined by cross-national principles. In parallel to the forces that have driven the globalization of the industry, however, there have been others that have resisted these developments and anchored the industry in national systems of healthcare delivery and consumption. This interplay between the global and the local is emerging as a predominant feature of the industry that is shaping its contemporary dynamics and will have significant consequences in the years to come. In this paper, I seek to explicate this development and examine the opportunities and challenges that it holds for healthcare providers and the policymakers who oversee the industry.
Healthcare: An Industry Unlike Any Other
The healthcare industry is distinctive in at least three ways. For one, in contrast to most other industries in which the ultimate goal of firms is profit-maximization, in healthcare this goal often poses a challenge to value creation through quality care. As an industry whose value creation lies in extending lives and enhancing their quality, there is a strong moral dimension attached to value creation, producing a delicate balance between this imperative and the different and often conflicting demands of economic performance and survival. Notwithstanding notable successes in combining value creation with financial goals, these goals often conflict with each other and impose tradeoffs. The vague notion of what is to be maximized challenges the development of performance measurement and creates scope for different points of view as to the appropriate indicators that should be used.
Further, the industry is characterized by distinctive structural issues. The consumers – patients with symptoms – are typically ignorant about the cause of their symptoms and the required treatment for relieving them; the suppliers – healthcare professionals, in affiliation with healthcare institutions or on their own, who diagnose the cause of the symptom, prescribe the treatment and may implement it – are, at least in the developed world, typically not paid by the consumers. Rather, market transactions involve one and often more intermediaries who administer the payment.[3] These intermediaries themselves vary in terms of their goals, agency and power, and their impact on the engagement between the healthcare provider and the patient receiving treatment.
Lastly, the healthcare industry stands out in terms of the demand for its output. Given the complex structure of the industry, identifying the actual source of demand is a challenge as it includes the patient, the doctor who prescribes the treatment and may implement it, and the payer for the service (at least in countries where the payers and the customers are two separate entities). Demand is often inelastic (what is the monetary value of life?) and is prone to information asymmetries of numerous kinds that influence the transactions and place much power in the hands of the intermediaries who pay for the service.
The distinctive attributes of the healthcare industry assume additional complexity as the industry globalizes. The ambiguity regarding the ultimate goal of healthcare, along with the subsequent difficulty of devising corresponding performance measures (notably whether performance should be measured by financial indicators, quality of care, outcome of treatment, or other metrics), are magnified by country-specific philosophies of life and mortality and varying perceptions regarding universal access. The United Nations (UN) Universal Declaration of Human Rights has long declared access to healthcare a basic human right: ‘everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care’.[4] Although more than half a century old, this assertion has not been adopted by all countries that are members to the UN in a comprehensive way. Variations in moral philosophy surrounding healthcare and the extent to which it is seen to be a universal right introduce stark differences in the healthcare industry across countries. These variations are reinforced by varying views of human ability to influence life quality and longevity versus those of faith and religion, including different perceptions of the value of life itself.
These philosophical and cultural differences bring about varying views as to who should be responsible for healthcare provision and who should pay for it. The UN International Covenant on Economic, Social and Cultural Rights assigned the responsibility for the provision of healthcare to national governments: ‘[every nation is responsible for] ‘the creation of conditions which would assure, to all, medical service and medical attention in the event of sickness’. [5] But this declaration has not been universally practiced. The size adjusted government expenditure on healthcare varies enormously across countries (Table 1). Country-specific approaches differ in terms of the ultimate provider and payer for healthcare, whether private or public, or as is the case in many developing countries – by the consumers. There are also considerable country differences in terms of access to healthcare services and its coverage. As the data in Table 1 show, out-of-pocket payment accounts for up to three quarters of total healthcare expense in countries such as Nigeria and India, but represents around a tenth or less of the total in many developed countries. These variations are accentuated by differences in the level of economic development and that affect the availability and quality of services (Table 1).
Table 1. Selected Healthcare Indicators by Country
Latest available: 2014-2016
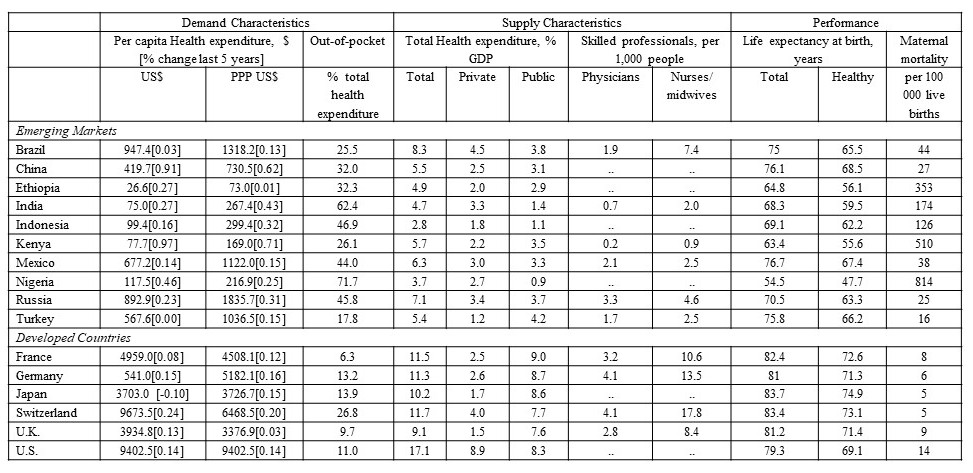
WHO, World Health Statistics http://who.int/entity/gho/publications/world_health_statistics/2017/en/index.html; World Bank Development Indicators Database
Country differences also express themselves in the nature of demand. Varying perceptions of healthcare versus healing by forces of faith and religion, coupled with different views of modern versus traditional medicine, often determine the level of demand for healthcare services and its nature. In addition, education levels influence information asymmetries between participants in the complicated transactions that define the industry. Lastly, differences in life style, diet, and other ongoing activities affect the types of diseases prevalent across countries and their frequency.[6] The data in Table 1 show vast variations in per-capita healthcare expenditure, indicative of these differences in the demand for healthcare across countries. In the following sections I discuss how the tension between the global and the local is shaping the nature of supply and demand for healthcare around the world.
The Tension between the Global and the Local: Demand and Supply for Healthcare Services
The forces that are driving the healthcare industry to become increasingly global and those that connect it to national systems manifest themselves within the framework described above. They are apparent in relation to both the demand for healthcare services and its supply. On the one hand, major participants in the healthcare industry, including healthcare professionals and institutions, drug producers, and consumers, have become more mobile, drawing healthcare delivery and consumption into global networks of interactions. At the same time, cultural, institutional, and behavioral differences continue to anchor the industry to different countries and arrest globalization.
Global and Local Demand
A major development that has globalized demand for healthcare is what has come to be known as ‘medical tourism’, that is, the travel by patients for medical treatments to other countries. While this phenomenon has existed for decades and by some accounts centuries, until recently it was small and confined to wealthy people from developing countries traveling to Western countries for medical treatment. What is new is the recent emergence of medical tourism from developed countries to emerging markets (Figure 1), driven by the development of local healthcare institutions in emerging markets and improvement in the quality of their healthcare services.
Figure 1. Medical Tourism
Destination countries by number of patients (in thousands), 2015
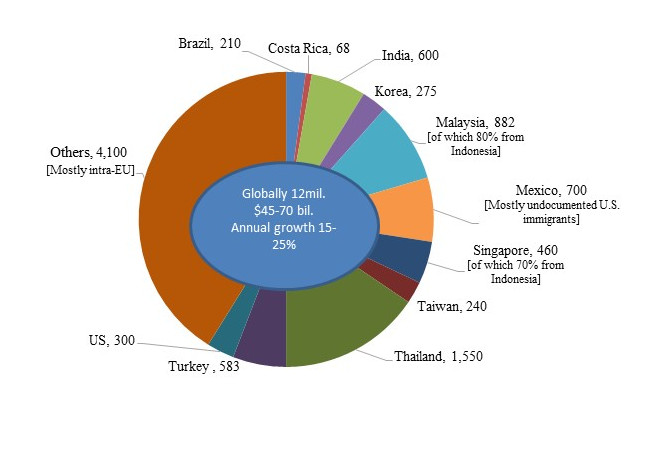
Patients Beyond Borders, http://www.patientsbeyondborders.com/medical-tourism-statistics-facts
Based on estimates by Deloitte, McKinsey, Gallup, the Economist, host countries health and tourism ministries
These institutions offer medical services for a fraction of the costs in developed countries (Figure 2) and minimal waiting time.[7] Combining a low-cost labor force with efficient delivery, assisted by state-of-the-art technology, hospitals in emerging markets have managed to cut costs and shorten delivery time to levels unimaginable in the developed world.[8] Accreditation by U.S. and Global Accreditation Associations provides quality assurance for patients and payers, and have removed major obstacles for the growth of medical tourism. By 2016 more than 600 hospitals worldwide were accredited by the Joint Commission International Accreditation, a number that has been growing by about 20% annually[9]. In 2015 medical tourism amounted for an estimated $40-$75 billion worth of economic activity, or about 1% of global healthcare expenditure.
Figure 2. Cost Variations of Medical Procedures
US$: 2015
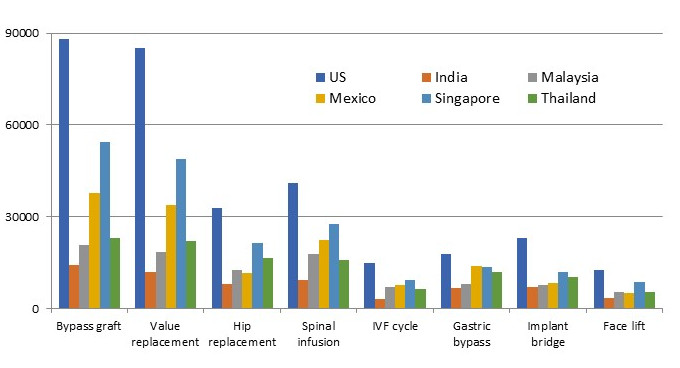
Patients Beyond Borders
The development of medical tourism has captured the attention of healthcare insurance services in the developed world. Large U.S. insurers have examined these offshore developments as low-cost alternatives for U.S. services, and some have incorporated them in their offerings. Britain’s NHS is considering partnerships with leading players in India and Thailand as a way to cut waiting times.
The growth in medical tourism suggests that at least in the short term, it offers solutions to limitations of healthcare systems in developed countries (i.e., high costs in the U.S. and long waiting lists in Europe). The long-term impact of this development on progress in addressing the causes that generate the demand for medical tourism is unclear. It appears likely that in the mostly privately-owned U.S. industry, competition from low-cost alternatives would create pressure for increased efficiency and lower costs, as I discuss in some detail below. This in turn could reduce demand for low-cost solutions elsewhere. The response of the government-owned healthcare system is Europe is more difficult to predict, as it less likely to be subject to market forces. European governments may opt for using medical tourism as a low-cost alternative that enables reduction of government resources allocated for healthcare rather than adding capacity to their local industries.
At the same time that demand for healthcare continues to expand globally, the type of demand varies significantly across countries, reflecting for the most part country variations in the prevalence of diseases. For instance, the number one cause of death in the developed world is heart disease, accounting for more than 12% of total deaths, whereas in mid- and low-income countries most deaths are caused by cerebrovascular disease (14%) and respiratory infections (11%).[10] Likewise, the incidence of cancer is three times higher in China than in India. The disparity in Africa is even greater.[11]
Global and Local Supply
On the supply side, the major providers of healthcare, notably healthcare professionals, hospitals, and pharmaceutical and other med-tech companies, have vastly broadened their global reach in recent decades. Movement of healthcare professionals, predominantly from emerging markets to developed countries, is not new, but its magnitude has grown considerably, fostered by reduction in traveling costs and liberalization of immigration policies for healthcare professionals. Initially, nurses came most commonly from the Philippines, but more recently, their national origins have widen considerably.[12]
These developments have often been driven by mismatches between supply and demand that have proliferated around the world – according to the World Health Organization (WHO) by more than seven million healthcare professional providers in 2016, a number that is estimated to double by 2035. More than two-third of the 300 respondents to the American College of Healthcare Executives’ annual survey reported experiencing shortage of registered nurses and primary care physicians, and more than half noted shortage of specialized physicians.[13] Leading U.S. hospitals have been importing nurses since the 1980s in the face of a large nursing shortage.
The movement of doctors across countries has also been prevalent, although less common than that of nurses due to different qualification requirements. According to one estimate almost 40,000 Nigerian doctors practice outside Nigeria, three-quarter of them in the U.K.[14] Whereas for the most part, these moves are initiated by individuals seeking to further their careers and better their lives, in some cases they are assisted by governments. For instance, the Cuban government, under the auspices of the WHO, exports local doctors to Brazil, pays their salaries, and receives payment for their services from Brazilian authorities, turning these transfers into a major source of the government’s foreign currency.[15]
Industry has a longer track record of global expansion. Pharmaceutical companies, in particular, have long been global. The high cost of drug development that gives rise to vast scale economies, coupled with short spans of patent protection, have pushed pharmaceutical companies to expand the market for their drugs across the globe.
Most recently, hospitals, which were traditionally deeply grounded in particular localities, also have started to globalize. Leading hospitals in emerging markets are rapidly expanding overseas. India’s Apollo Hospitals Group, the largest private hospital group in Asia, operates 55 hospitals with 9,215 beds, and has facilities in India, Sri Lanka, Bangladesh, Ghana, Nigeria, Mauritius, Qatar, Oman, and Kuwait, and plans for further global expansion. Only regulations have prevented it from entering the U.S. [16]. Some of the most prestigious U.S. hospitals, among them Johns Hopkins, Cleveland Clinic, Harvard, and Duke, have formed partnerships that offer combined treatments in the U.S. and overseas. Similarly, Canadian hospitals such as SickKids Children’s Hospital have begun to expand internationally.
The major barrier for the globalization of healthcare supply is country regulations. Doctors are tied to the locality in which they receive their medical training by varying qualification requirements that raise the cost of movement across countries. Foreign hospitals’ expansion is also limited by country restrictions, making this segment of the healthcare sector the least global. The share of FDI in healthcare services is a fraction of total service FDI in both developed and developing countries, although it registered substantial growth over the last decade. In an era where cross-border M&A activity has been mushrooming across industries, there has been almost no cross-border acquisitions of hospitals (although domestic mergers are common).[17]
U.S. hospitals and other healthcare providers have been among the world’s most active foreign investors, particularly in Latin America and the U.K.[18]. The Federation of America Hospitals lists almost a hundred overseas hospitals owned by U.S. major hospitals. However, there is no corresponding activities the other way around. For instance only regulations prevented Indian hospitals from establishing themselves in the U.S. Whereas countries around the world, most notably developing countries, have become increasingly open to foreign ownership of healthcare services, the U.S. has been highly restrictive.
Regulations and country variations have been a drag also on the global expansion of pharmaceutical companies. The regulatory environment that surrounds drug development, testing, and approval varies considerably around the world, undermining advantages of global scale. Varying levels of patent protection across countries are another challenge for the globalization of pharmaceutical companies, and variations in diseases and their prevalence impact global standardization of drug development.
Implications for the Healthcare Industry
As the home of some of the world’s most prestigious hospitals and healthcare professionals, developed country institutions and professionals are well-positioned to benefit from the globalization of the healthcare industry. Global developments increasingly make it possible to scale the reputation of hospitals and professionals globally and exploit them on a global scale. It enables local institutions in these countries to attract patients from around the world to their existing facilities and increase their share of the rapidly growing medical tourism. As emerging market consumers become wealthier, demand for high quality healthcare services in these countries is increasing, and could foster medical tourism to developed countries.
In addition to attracting patients to developed countries, these constituencies should also be able to expand their scope globally by establishing themselves overseas, by either direct investment or through various forms of partnerships with local providers in foreign countries. This process will vary according to the type of services provided and their comparative advantage in different countries.
Some reputable U.S. hospitals have recently been experimenting with such endeavors, and would likely pursue these further as a means to leverage on their expertise and increase market share. The Directory of U.S. Hospital Partnerships with Foreign Hospitals, published by the American College of Healthcare Executives and the American Hospital Association, lists dozens of partnerships. To qualify for inclusion in the Directory, partnerships need to be deep and comprehensive, and form ‘a cooperative and mutually beneficial relationship between a U.S. hospital and a hospital in a different country, … designed to facilitate the exchange of knowledge, technical information and other insights that contribute to improved healthcare services in both hospitals.’[19]
At the same time, global developments could also pose considerable challenges to hospitals and healthcare professionals in the developed world. The forces that enable them to broaden the potential market for their services also increase cost pressures and put them in competition with low-cost providers. These constituencies, notably in the U.S., have little experience in cost-driven competition and this could pose a serious challenge for them. The strongest impact of these forces will probably be felt in what are today the most lucrative parts of the industry, namely the highest cost operations and procedures. The high cost of these treatments compared to the emerging alternatives overseas will increase the incentives to travel elsewhere. These developments will put pressure to improve the consumer experience (for instance, by providing rehabilitation facilities for medical tourists and accommodation for accompanying relatives) and at the same time cut costs in order to stay competitive.
The challenge for these constituencies lies in designing strategies that are responsive to the tension between the global and the local that I outlined in this paper, and take advantage of them by articulating the appropriate balance, considering their distinctive sources of strengths and weaknesses. The rewards for doing this properly are vast.
References
- This paper is derived from a course on the globalization of healthcare developed and taught by Professor Nachum as part of Baruch College MBA program for Healthcare professionals. An earlier version of this paper appeared as Baruch College’s Weissman Center Occasional Paper, 2018. The author acknowledge with deep gratitude the excellent comment of the Editor during the review process.
- The health care industry is defined broadly to include health care professionals (e.g., doctors, nurses), healthcare institutions (e.g., hospitals), pharmaceutical companies, and producers and suppliers of equipment for healthcare.
- This is the common practice in developed countries. In developing countries large share of healthcare costs is covered by the consumers, as will be discussed below.
- Article 25, 1948
- Article 12, 1966
- Farmer et al., Reimagining Global Healthcare: An Introduction. 2013; Holtz C. (ed.), Global Health Care: Issues and Policies. 2017; Reid, The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care. 2010.
- Siciliania, Moranb and Borowitz. Measuring and comparing health care waiting times in OECD countries. Health Policy, December 2014
- Wall Street Journal, The Henry Ford of Heart Surgery: a Factory Model for Hospitals. November 25, 2009; Hub and Spoke, HealthCare Global. Harvard Business School Case #313030, 2015.
- Joint Commission International https://www.jointcommissioninternational.org/about-jci/jci-accredited-organizations/
- World Health Organization (WHO), The Global Burden of Disease Project.
- International agency for research on Cancer, http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx
- Brush et al., Imported Care: Recruiting Foreign Nurses to U.S. Health Care Facilities. Health Affairs 2004
- http://www.ache.org/pubs/research/ceoissues.cfm
- https://www.vanguardngr.com/2017/12/medical-tourism-ambode-harps-retraining-medical-practitioners/
- https://www.nytimes.com/2017/09/29/world/americas/brazil-cuban-doctors-revolt.html?_r=1
- Health City Cayman Islands. Harvard Business School Case #714510, 2014.
- Holden, C. The Internationalization of Corporate Healthcare: Extent and Emerging Trends. Competition & Change, 2005, 9(2), 185-203; Holden, C. The Internationalization of Long Term Care Provision. Global Social Policy, 2002, 2(1), 47-67; Herman L. Assessing International Trade in Healthcare Services. The European Centre for International Political Economy Working Paper No. 03/2009, Brussels 2009.
- Jasso-Aguilar, R. et al. Multinational corporations and health care in the United States and Latin America: strategies, actions, and effects. Journal of Health and Social Behaviour, 2004, 45, 136-157.
- https://www.ache.org/foreignhospitaldirectory.cfm
CEASE: Community Empowerment to Address the Substance-Use Epidemic
Elisha M. Friesema MBA, Stephen Palmquist, Prachi Bawaskar MS, MBA, Medical Industry Leadership Institute, Carlson School of Management, University of Minnesota
Contact: Elisha M. Friesema, fries202@umn.edu
The 2018 BAHM Case Competition, held at the University of Miami School of Business, focused on business-based policy solutions to the national opioid crisis. Student teams from the University of Minnesota, University of North Carolina at Chapel Hill, and the University of Toronto took the top three places.
Acknowledgements: The authors thank their faculty advisors Drs. Archelle Georgiou and Mike Finch, the Medical Industry Leadership Institute at the Carlson School of Management, and the Minnesota Department of Health for their support.
Disclosures: The authors have no conflicts of interest to disclose.
Abstract
What is the message?
What happens if a salmonella outbreak is suspected? Officials determine that this is not an isolated incident, then confirm it is salmonella making people ill, and detect the cause – most recently this was romaine lettuce. Hence, we find the point of origin and then control it by making sure its removed from all restaurants and store shelves to prevent more people from being exposed. This contagion model has also been successfully applied to social epidemics such as gun violence in Chicago.
This article discusses how to take these principles and reframe the way we think about and treat opioid use. Minnesota sees almost 400 opioid-related deaths each year. [1] There are concerted efforts underway to address the supply of opioids, both through provider prescription and drug seizures. Our solution, CEASE, attacks demand by bringing resources and support to those most at risk.
What is the evidence?
Review of analogous programs that have reduced gun violence in multiple cities.
Submitted: June 30, 2018. Accepted after review: July 31, 2018
Cite as: Elisha M. Friesema, Stephen Palmquist, Prachi Bawaskar. 2018. Community Empowerment to Address the Substance-Use Epidemic. Health Management Policy and Innovation, Volume 3, Issue 2.
Background
Opioids have been in use for hundreds of years, but it was not until the 1990’s that pharmaceutical companies and patient advocacy groups began promoting their widespread use. In 2001, the Joint Commission declared pain to be the fifth vital sign, which some view as a trigger for providers to prescribe opioids more aggressively. [2] As excessive use built up, more potent opioids were sought out ultimately leading to the declaration by President Trump that the opioid epidemic is a public health emergency. [3]
Within Minnesota most opioid-related deaths are centered in a handful of counties. Prescription opioids are more likely to be used by 45- to 54-year-olds whereas 25- to 34-year-olds are more likely to use heroin. [1] As heroin use continues to rise, we anticipate the average age of death to decrease. We chose to focus on Hennepin and Ramsey counties, which are home to the Twin Cities of Minneapolis and St. Paul, which represent 44% of Minnesota’s deaths.
Profile and Risk Factors for Opioid Dependence
Risk factors for the development of a substance use disorder accumulate over a lifetime and range from genetics, substance exposure during pregnancy, adverse childhood events during infancy and early childhood development, early exposure to drugs, and drug-usage in social contexts during high school. Additional factors are directly related to social determinants of health and include a lack of a livable wage, safe housing, quality education, health insurance coverage, social support, and social cohesion. [4]
Numerous studies have examined the epidemiology of substance use disorders to understand the factors driving initiation of opioid use. Research repeatedly shows that social and familial networks containing an illicit drug user are the strongest single predictor of illegal drug use in an individual. [5] Consequently, substance use bears similarities to a contagious disease; moving from contact to contact, illicit drug use spreads through social and familial networks ensnaring people and their communities. Thus, preventing a person’s first exposure to prescription opioids can significantly decrease their likelihood of becoming addicted in the future.
After initiation, it is essential to understand the risk factors that lead to an overdose. The main known risk factors include: high dose of prescription opioids (over 50 morphine milligram equivalents), using benzodiazepines or alcohol concurrently with opioids, taking long-acting opioids, using prescription opioids that are not prescribed to the user, using opioids after a period of sobriety, using heroin, fentanyl, synthetic opioids, or having a previous non-fatal opioid overdose. [6]
Continued use is another concern as it can lead to physical dependence and often results in loss of employment, insomnia, troubled relationships, societal isolation, depression, anxiety, and suicidal thoughts. [7] These factors echo those identified in the social determinants model that influence why an individual may start using opioids in the first place, suggesting that a substance use disorder can send an individual into a spiral of use from which it becomes increasingly difficult to recover.
Supply
Opioids reach consumers through several mechanisms. An individual can receive a legal prescription from a medical practitioner and fill it at a pharmacy. Legally prescribed pills can also be given or stolen by friends or family members or sold illegally “on the street.”
Illegal opioids have multiple channels. Heroin flows into Minnesota from Mexico up Interstate 35. Fentanyl and fentanyl synthetics are often manufactured in China and shipped through Canada into the United States via the mail service. [8] This is particularly problematic as fentanyl is not currently detectable by traditional screening methods and is easy to obtain. It took our team less than two minutes before we were entering credit card information into a website guaranteeing delivery of hydrocodone to our office.
Current Efforts to Curb Supply
There are significant efforts by both the federal and state governments to curb the supply of opioids. Law enforcement focuses on seizures and arrests, while public health officials emphasize campaigns such as drug-take back days and drop boxes. In a local effort, Hennepin county committed to having every first responder carry Naloxone.
Providers and health systems have also made dramatic efforts to curb inappropriate prescribing across the country and are implementing quality improvement efforts including benchmarking and peer comparisons. Minnesota providers have driven their rates down almost 10% annually. [4] Providers are required to register for prescription monitoring programs, but not yet required to monitor lists prior to prescribing.
Efforts to re-educate and train providers are also underway. These mostly target dentists, who are the largest class of inappropriate opioid prescribers. Along those lines, there are efforts to decrease first time prescribing. We know that the earlier a person is exposed to opioids, the more likely they are to have a substance use disorder in the future.
What Are the Gaps in Minnesota?
It is clear that Minnesota is tackling many aspects of the opioid crisis, but there are significant gaps in the current approach. Most significantly, weaknesses exist in:
- Reactive: Waiting for the individual to either seek treatment on their own or have a medical emergency requiring intervention rather than proactively seeking them out
- Uncoordinated: Lack of coordination between community entities to connect an individual with the resources they need despite willingness to work collaboratively across sectors
- Individual-centered: A lack of concerted effort to stop the spread of drug use through social and family networks
Proposed Solution
Fortunately, there is a proven approach that empowers communities to solve complex issues that span medical, social, economic, and cultural realms. An adaptation of epidemiologist’s Contagion Model, under the name ‘The Cure Violence Model,’ has been successfully implemented to address gun violence in cities across the country over the past decade, many of which make the news every day, including Baltimore, New York, and Chicago. The contagion approach helps isolate, contain, and resolve conflicts that lead to gun violence. Independent evaluations show a 41% to 73% decrease in shootings and killings in targeted neighborhoods. Critically, 95% of parents who interacted with Cure Violence reported it making them better parents indicating a ripple effect on the entire community, influencing beyond the primary target of gun violence [9]. By adapting this approach, CEASE can act as a convener for the existing resources for individuals and families and address demand for opioids.
Cure Violence Model
The Cure Violence Model uses the core principles of curing infectious diseases to address the problem of gun violence. Instead of using a law enforcement-based approach, the model addresses the social issues that significantly contribute to violent behavior. [10] The Cure Violence team identifies at-risk individuals and provides resources at both the individual and community level for identifying ways to resolve conflicts.
Cure Violence uses a three-step approach to prevent violent crime by 1) impeding the spread of violent behavior, 2) diagnosing and changing mindset of potential at-risk individuals, and 3) providing alternate solutions to violent crime. [10] The model’s success is attributed to four features.
- Works independently of law enforcement without impeding their work
- Addresses root causes of violence
- Collaborates with existing community resources and structures
- Empowers the community by focusing on hiring community members in pivotal roles
The focal points of the model involve identifying at risk groups, tracking violent acts in the community, and quickly deploying “Violence Interrupters”, who are hired staff from the community, trained to diffuse situations and help at-risk individuals find the resources they need. Many Violence Interrupters have a personal history with violent crime, including being former gang members; they are now critical leaders in the community.[11]
The CEASE Model
The CEASE (Community Empowerment to Address the Substance-use Epidemic) model focuses on individuals who are currently addicted, those in remission, and those who are at risk for future use. With this, we detect the hotspots and dedicate resources to them to isolate and treat those in need. We then engage the community to ensure the epidemic it does not spread.
Establishing Hubs
Applying the foundational principles used in the Cure Violence Model, community offices, or “hubs,” will be established within neighborhoods to address the different social determinants of health for the identified group. Data feeds from multiple sources will identify the areas at highest risk in real time so that community hubs can be established to isolate opioid misuse. A Data Analyst will work with the coroner’s office and law enforcement to build a real-time heat map and demographic database containing drug overdose deaths, overdoses, and arrests. This will provide the organization the ability to flex resources quickly to respond to community needs. 2016 death data from Minnesota Department of Health and Hennepin County Coroner’s office show that only a handful of zip codes are contributing to the high number of deaths seen in Hennepin County (Figure 1). With a full time data analyst and strong community connections to law enforcement, medical entities, and the coroner’s office, future data can pinpoint exact addresses of overdoses, deaths, and opioid related arrests. This data will allow for specific placement of CEASE hubs.
Community workers will work to identify individuals and provide crisis intervention when someone is at risk for relapse or just had an overdose. They will meet those at highest risk where they are, rather than waiting for them to come to CEASE, and will connect them with existing community resources to address their social determinants of health. The hub will act as a center for the entire community, raising awareness, creating a support center, and ultimately decreasing the stigma often attached to opioid-use-disorders.
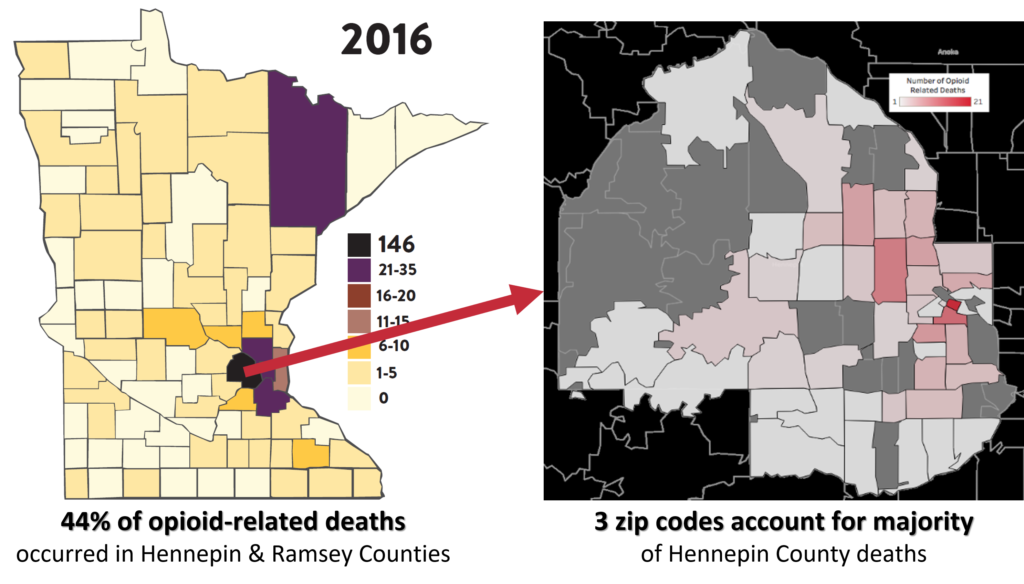
Key Activities
Safe and healthy communities develop by changing behavior and disrupting the status quo. Key activities engage high-risk individuals, teach coping skills to avoid opioid use, and enable access to resources. Community outreach programs, advertising, events, collaboration with community groups, and positive law enforcement relations will increase awareness and empower communities to change in the status quo. These activities will result in outcomes that decrease socioeconomic stressors and allow participants to avoid opioids, overcome stereotypes and become productive members of their community.
As discussed earlier, CEASE will connect individuals with community services as needed using a hub-and-spoke model with the individual in need at the center and a CEASE employee by their side. Together they will evaluate the individual’s need for specific services “spokes” to reduce stressors that affect substance users and allow them to drive the needed change in their lives. The eight individual spokes of community services include transportation, food, housing, education, job training, employment resources, medical care and mental health, and combating social isolation.
The face of CEASE, and the critical factor that differentiates it from current efforts to address the opioid epidemic, are the Community CEASE Workers. Many individuals who are in this role have a history of substance use disorder and live in the community, so that they can be accessible – physically and emotionally – to the individuals in the community. This background and experience will help establish trust and position CEASE as a safe space to seek help.
The Community CEASE Workers will be trained on motivational interviewing and cessation discussion strategies. They will be knowledgeable in ascertaining clients’ needs and in connecting them to available community resources. CEASE workers will also work preventively with families and friends of individuals battling this disease, to ensure strong support networks and inhibit the contagious spread of substance use. Additionally, these community resource workers will raise awareness and create collaborative coalitions with existing community entities to better combat the opioid epidemic.
The hub will also house a group of nurse practitioners and medical assistants trained in treating chemical dependency. To establish the highest level of trust and minimize as many barriers as possible, these medical teams will work in the hubs and connect with specialized medical facilities as needed.
The greatest strength of our model is the capacity to flex services depending on the particular needs of the community and each individual:
Example 1:
- Maria Smith: High functioning executive, mother of 2; in remission for 16 weeks
- Crisis: Recently lost her job as a CFO
- Intervention: The team will help address employment and social support. Within the social network, we will isolate anyone who is currently using or also at high risk. Next, we will address his immediate needs. Maria needs to feel like she is not alone in this. She needs a new job, to have income to keep a roof over her daughters’ heads and food on the table. CEASE will address the root causes and stressors that could drive her to relapse.
Example 2:
- Joe St. Paul: Current heroin user
- Crisis: Has just been admitted to a local ER for a heroin overdose, has been arrested in the past for possession of illicit drugs, is sleeping at friends’ houses, and has not been regularly employed in over a year
- Intervention: Because of CEASE’s relationship with the hospital, they notified us so we could seek him out. CEASE engaged his existing support network and identified anyone at risk of hindering his recovery. Given Joe’s situation, he needs assistance in almost every area so we bring in a team to help.
- An advanced practice nurse helps address his medical needs, getting him started on MAT.
- A social worker helps to get him into a local long-term shelter to provide a safer more stable environment as well as consistent meals.
- Our case manager checks in with him daily just to see how he’s doing and to remind him we are there for him and that there are group sessions being held several times that day and we hope to see him at one.
- Once Joe has reached remission, the team will begin to address other areas, like employment, education, and consistent transportation.
Organization Structure
CEASE will be a formally organized as a 501(c)3 non-profit organization with the following vision and mission:
Vision: CEASE will free individuals, families, and communities from the harms inflicted by substance use disorder.
The three strategic themes within this vision are to:
- Reduce the number of deaths caused by substance use
- Reduce the number of individuals suffering from substance use disorders through prevention of initiation and cessation.
- Create a sustainable, scalable, and replicable community empowerment model to address substance use across the Twin Cities that could be adapted for other sites
The organization will have a traditional non-profit structure with a Board of Directors, which will provide strategic direction and oversight, and a management team responsible for operational execution. The board will be comprised of a diverse group of key stakeholders and key opinion leaders from different sectors of the community.
Key staff will include:
- Chief Executive Officer
- Communications and Marketing Director
- Operations Director
- Data Analysist
- Business Development Director
- Human Resources Director
- Finance Director
Under the direction of the operations director, each hub will employ:
- Community Service Manager
- Community CEASE Workers
- Case Coordinators and Social Workers
- Nurse Practitioner
- Medical Assistants
Stakeholder Commitments
This success of the CEASE model requires buy-in, cooperation, and integration with multiple stakeholders. Engagement with the Minnesota Department of Health is a first step as it will act as a crucial partner organization. The Department’s existing relationships with county social services organizations will provide foundational support for CEASE.
Subsequently, other organizations will be engaged to provide the resources necessary to provide each of the model’s spokes. Initially, these will include: Hennepin Health, Fairview Health, Metro Transit, Aeon, Catholic Charities, MN Career Pathways, HIRED, Avivo, Lutheran Social Services, Second Harvest Heartland, Minnesota and St. Paul Sheriff’s offices, Tubman, and Hazelden Betty Ford Drug and Alcohol Addiction Programs. These organizations provide vital services in each of the spokes and are trusted and respected resources in the community. Creating a centralized resource for at-risk populations will increase access and reduce frustrations in an already resource-poor environment.
Implementation and Tracking Success
To ensure operational efficiency, CEASE will be implemented through a phased approach. Phase 1 will consist of a single pilot hub in one of the hardest hit zip codes in Hennepin County (55403). Through this, CEASE will learn from and continuously improve upon our model and practices, before scaling up to serve our entire target community. Phase 2 will expand to a total of 10 hubs across Hennepin and Ramsey counties. Phase 3 will further extend beyond our community to 25 hubs across the country.
Determining the effectiveness of the CEASE model will involve several evaluation metrics. The primary outcome will be the number of opioid-related deaths in Hennepin and Ramsey counties. Secondary measures will include the number of emergency department visits for opioid overdose in Hennepin and Ramsey counties, the number of arrests by law enforcement for opioid possession, and utilization and satisfaction rates of CEASE community hubs.
Program Cost
The estimated CEASE’s annual program cost for phase 2 is approximately $13 million. We arrived at this estimate by using median salary information for each desired position from the Bureau of Labor Statistics or non-profit survey data, adding overhead costs per employee, and estimating the number of staff needed to support our model. We assumed ten community hubs will be needed across the Twin Cities area based on heat map data. To estimate office and overhead costs we found a median cost of renting commercial space in Minneapolis to be $22 per square foot. Based on the number of community workers needed to implement the Cure Violence model in several large cities across the United States [12], we estimate the need for 80 community CEASE workers. Additionally, Cure Violence estimates that the average cost of implementing their model ranges from $10 to $13.3 million, further justifying our cost estimate. [13]
Funding
Due to the length of time and complicated process needed to secure government funds for a project of this magnitude, we recommend three approaches to obtain the necessary funds. Each method can independently fund this community intervention.
Federal funding: Our first target would be grants from the money allocated by the Trump Administration to combat the opioid crisis. Next year alone, the Trump Administration has requested $625M in funding to be given out to states and we propose receiving the necessary $44M to run our program for a minimum of 4 years. [14]
“Penny-a-Pill” Fee: A new stream of state-level revenue from a one-cent stewardship fee on every morphine milligram equivalent of opioids dispensed in Minnesota. While this revenue stream would be an entirely new source of funds, the one-cent fee has broad support in Minnesota and has been endorsed by the governor and state legislators. [15] State government analysis shows that this revenue stream would generate $20 million a year. [12] Our organization would apply for funding from this revenue stream.
Extension of the expiring Minnesota provider tax: Our third revenue stream recommends the continuation of an existing medical tax that is set to expire. Since 1991, Minnesota has had a 2% tax on providers, levied explicitly on the revenues of hospitals, providers, pharmacies, and wholesale drug distributors. This tax has historically funded expanded medical insurance for low-income citizens. In recent years, the funding of expanded medical coverage has shifted towards general taxation, making the sun-setting of this tax more feasible. Currently, this tax raises $700 million a year and is set to expire in 2020.[16] Even if the tax is reduced to 1%, we would still be asking for less than 10% of the revenue. Much like the one-cent fee on opioid pills, this law would require action by government bodies to extend an existing tax, which may be difficult and require interim ways to fund the program. Additionally, both provide a way for those who are partially responsible for creating this epidemic to directly contribute to its solution.
Impact Analysis
To evaluate the societal economic impact of our community intervention we created a break-even cost and a projected impact model. To value the impact of treating an individual we have used the estimated cost to society of an individual with opioid use disorder as used by the Minnesota Management and Budget, which is $309,020 per year. [17] The break-even point for phase 2 occurs through assisting 42 individuals into remission. Beyond that, we would have a societal surplus.
Looking at estimates of what is achievable given the success of the Cure Violence model in cities across the globe, the lowest results seen in any particular city, after full implementation, is a 41% drop in shootings and killings. [9] Using this as a target value, we estimated the net impact of our program if we could achieve a 30, 40, or 50% decrease in the number of opioid addicted individuals in our target community (Figure 2). Of note, the number of opioid dependent individuals in our target community is unknown, but survey data has shown that for every person who dies from a drug overdose, there are 115 people abusing opioids in the community [18]. Using this methodology, we estimate the value of this program to our community could exceed $2 billion.
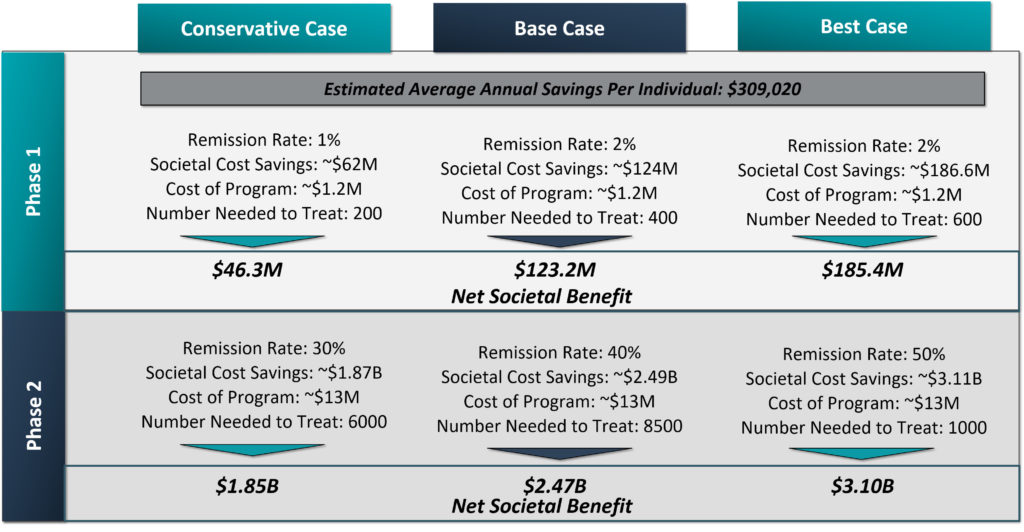
Conclusion
Spreading like an infectious disease through our country, the opioid epidemic is ravaging communities across the U.S. In Minnesota’s Hennepin and Ramsey counties alone there were 175 opioid overdose deaths in 2016 — that number is expected to rise. Geocoding analysis, along with the epidemiological research, reinforces our conclusion that substance use disorder spreads through family and social networks, much like a public health epidemic. From our review of community resources and community initiatives, there are definite plans to address many aspects of the opioid epidemic. The significant gap within this community remains a lack of coordinated resources to attack the root causes of why an individual begins using and does not quit.
CEASE addresses the root causes of substance use by empowering the community to identify those at risk and get them the resources they need. With the societal and political desire to solve this critical issue, we believe that CEASE would get the funding it needs, especially given its potential cost savings to society. Furthermore, after full implementation, our community intervention has the ability to scale to communities across the country.
References
- Wright, N., Roesler J. Drug Overdose Deaths among Minnesota Residents 2000-2016. Minnesota Department of Health Injury and Violence Prevention Section: Minnesota Department of Health;August 2017.
- Baker DW.The Joint Commission’s Pain Standards: Origins and Evolution. The Joint Commission;2017.
- President Donald J. Trump Is Taking Action on Drug Addiction and the Opioid Crisis. In: House TW, edOctober 26, 2017.
- Indicator Dashboards Opioid Dashboard. The Minnesota Department of Health. www.health.state.mn.us/divs/healthimprovement/opioid-dashboard/#NumberPrescriptions. Published 2018. Accessed March 11, 2018.
- Galea S, Nandi A, Vlahov D. The social epidemiology of substance use. Epidemiol Rev. 2004;26:36-52.
- Prevention & Control Opioid Overdose. Minnesota Department of Health. www.health.state.mn.us/divs/healthimprovement/health-information/prevention/opioid.html. Accessed March 11, 2018.
- Bennett M. The Great USA Opioid Epidemic with Expert Insight. In. ConsumerProtect.com2017.
- Scott D. This Is How Easy It Is to Order Deadly Opioids over the Internet. In. Vox: Vox Media; 2018.
- Cure Violence. Scientific Evaluations. Cure Violence. http://cureviolence.org/results/scientific-evaluations/. Accessed March 11, 2018.
- Butts JA, Roman CG, Bostwick L, Porter JR. Cure violence: a public health model to reduce gun violence. Annu Rev Public Health. 2015;36:39-53.
- Cure Violence. Annual Report 2014. Cure Violence;2014.
- Butts J. Evaluating the Cure Violence Model in New York City. John Jay Research and Evaluation Center;2016.
- Cure Violence Admin. Policies to Cure Violence. In. News & Events. Vol 2018: Cure Violence; 2013.
- An American Budget, Fiscal Year 2019. In: House TW, ed. www.whitehouse.gov2018.
- A ‘Penny-a-Pill’ to Fund Opioid Treatment and Prevention. In: Office of Governor Mark Dayton SoM, ed: Office of Governor Mark Dayton; 2018.
- Carlson HJ. Bill Would Keep Medical Provider Tax in Effect. In. The Post Bulletin. PostBulletin.com2016.
- Merrick W, Elder T, Bernardy P. Adult and Youth Substance Use Benefit-Cost Analysis. mn.gov: Minnesota Management and Budget;2017.
- Registration Support. DEA Diversion Control Division. https://www.deadiversion.usdoj.gov/. Published 2018. Accessed March 11, 2018.
A Blueprint for Developing Leadership in Physicians and Non-Physicians
Gregory P. Shea, Ph.D., M.Sc., Jeffrey P. Kaplan, PhD, and Stephen K. Klasko, MD, MBA
Contact: Gregory P. Shea, sheag@wharton.upenn.edu
Abstract
What is the message?
This article outlines a comprehensive approach to designing and evaluating leadership development programs for physicians and non-physicians in Academic Health Centers, including a description of the program design, approaches to assess the program impact, and the results of a combined evaluation of the program’s impact over three years.
What is the evidence?
T1 and T2 administration of the ESCI (Emotional Social Competence Index) 360 instrument and questions on a confidential, end of program evaluation completed separately by the program participants and by their respective sponsors (generally their supervisors) concerning various aspects of the program including its overall value, as well as confidential surveys concerning value of stretch assignments, and the evaluation of individual program sessions.
Submitted: May 18, 2018; accepted after review: July 20, 2018
Cite as: Gregory P. Shea, Jeffrey P. Kaplan, Stephen K. Klasko. 2018. Developing Leadership in Physicians and Non-Physicians. Health Management Policy and Innovation, Volume 3, Issue 2.
Leadership Development in Academic Health Centers
Calls for leadership development in medicine such as those made by Lerman and Jameson (2018) occur within the context of many Academic Health Centers that have or have had such programs.[1] Lucas, et. al., (2018) reported on the prevalence of leadership development programs (LDPs) in Academic Health Centers, with 93 of 94 survey respondents indicating that their institutions provided some type of leadership training and 61 indicating the existence of a formal internal program. In the authors’ opinion, the prevalence of such training and programming did not, however, match rigor in the evaluation of such efforts: “…programs should incorporate more rigorous evaluation beyond satisfaction surveys and strive to find meaningful outcome measures…” [2] (p. 8)
Healthcare providers, educators, and researchers face a turbulent and uncertain environment. Market consolidation of both insurers and providers contribute at least as much to the mix in Philadelphia as elsewhere. Jefferson Health, of course, exists in that environment and has pursued large-scale change both internally (e.g., leveraging technology to better deliver care and education) and externally (e.g., expanding dramatically in size and reach through mergers). Hence, the leadership challenges have centered on developing a new Jefferson, redesigned in its clinical and its business processes and far greater in its size and reach. The Jefferson Leadership Academy was designed to develop enhanced leadership capacity in general and in particular, leadership of change among those in significant organizational roles (albeit not senior leaders) and likely to occupy more significant roles in the future. Findings indicate an impactful program, thereby suggesting a program design for use by others seeking to develop physician and non-physician leadership in academic health systems and in a way that positively impacts the organization.
Program Design
Just over 30 participants began 10 months of classroom work each year, over half of them physicians. Selection began three months earlier and included participants being sponsored (usually by supervisors), completing a several page application, and senior level review. Pre-class work involved a four-way meeting (participant, sponsor, and two program leads—one internal to Jefferson and one external) to reinforce expectations about the course and its demands, as well as to review developmental objectives and possible stretch assignments. Classroom work entailed a full day (at least 8-5) each month. Topics included finance, change leadership, teaming, negotiation, emotional intelligence, diversity and inclusion, marketing, and creativity. Faculty included Jefferson personnel and numerous nationally recognized topic experts. Participation, application sessions, and role play characterized significant portions of classroom work. Session design included special attention to continually ‘shuffling the deck’ in order to maximize networking among program participants. A presentation to and discussion with sponsor and senior management concluded the course. The CEO provided regular and public support of the program (e.g., conducted a session opening the program, attending the program conclusion, and providing funding).
Stretch assignments comprised the second leg of the program and overlapped with the program but did not necessarily begin or end with the classroom portion of the program. Stretch assignments were to include – and, generally, did include – ‘real work’, i.e., work that needed doing, work that mattered to both the participant and to his or her sponsor, and that required the participant to labor outside of his or her normal set of duties and involve others in doing so. Restated, assignments that a participant might do on his or her own or that might only necessitate involvement by current colleagues or staff, would not meet criteria for a good stretch assignment.
Thirdly, and importantly, each participant received two one hour executive coaching sessions each month with a veteran external coach over the final six months of the program. The coaching process included two three-way meetings of sponsor, participant, and coach, initially to set up the coaching process and objectives, and again at the end of the six months to close down the process and to identify next steps. Each participant worked with his or her coach to create a leadership development plan which identified competencies, behavioral objectives, action plans, and metrics. The same executive coaches served as coaches throughout the three years of the program. Inputs to the coaching process included the the Emotional and Social Competence Index, or ESCI, Hogan profile, stretch assignments, participant developmental agenda, and daily work challenges.
Finally, regular ‘crosstalk’ occurred by design among the program staff designing and delivering each of the three aspects of the program. This crosstalk occurred during design, delivery, and debriefing of the program to maximize program integration and focus.
The program design changed minimally over the three years measured.
Measuring Program Effectiveness
Measures of participant leadership skill development were T1 and T2 administration of the ESCI 360 instrument and questions on a confidential, end-of-program evaluation completed separately by the program participant and by their respective sponsors (generally their supervisors). Questions on an end-of-program evaluation completed separately by the program participant and by their respective sponsors (nearly always their supervisors) concerned various aspects of the program including its overall value. Other confidential questioning concerned the value of stretch assignments and the evaluation of individual program sessions. Further measure of program value came from an unanticipated measure.[3]
The Emotional and Social Competence Index, or ESCI, is a 360 degree feedback instrument. It was administered early in the program (in months 2-3) and then again 12 months later, i.e., approximately six months after the program concluded. The initial administration corresponds with the advent of six months of bi-weekly executive coaching, and the second administration provides a way of maintaining participant and sponsor developmental focus. In other words, about one year separated T1 and T2, a gap corresponding to the generally accepted minimum amount of time necessary for behavioral changes to occur and to be noted by others.
The ESCI is a multi-rater coaching and development instrument based on emotional intelligence (EI) research. It is designed to facilitate how people understand how others see them, both strengths and weaknesses, within the domain of EI. Twelve scales comprise the ECSI: achievement orientation, adaptability, coach and mentor, emotional self-awareness, emotional self-control, empathy, influence, inspirational leadership, organizational awareness, positive outlook, and teamwork. Korn Ferry owns and distributes the ESCI.
Raw descriptive statistics provide were collected on all measures. 53 of 95 participants or 56% were physicians.
Outcomes
The distribution of T1 and T2 differences in ESCI data met the requirement for paired t-testing, namely it approximated a normal distribution across all categories and all raters. The data for all three cohorts were analyzed to determine statistical significance at the .05 level (using both one and two tailed testing) between T1 and T2 scores, i.e., of the scores at the beginning of the course (i.e., between 2 and 3 months after the beginning of program course work) and the scores approximately 6 months after the end of the course, a calendar time of approximately 12 months. The raw score differences across all years appear graphically in Figure 1 below. Testing for statistical significance by grouping all T1 and T2 scores from all three cohorts combined led to the finding of differences statistically significant at the .05 level for one and for two tailed tests for all 12 competencies. The largest gains were in the areas of (in descending order): Inspirational Leadership, Influence, Emotional Self-Awareness, and three tied (Conflict Management, Coach and Mentor, and Organizational Awareness).
Figure 1: ESCI t1,t2 Average Raw Scores by Competency Averaged Across Cohort
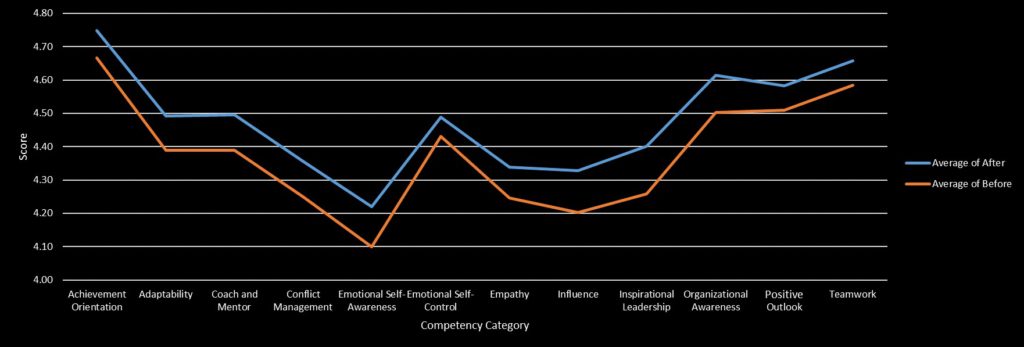
Participants completed a confidential end of program survey. On average, using a seven-point scale, participants, by cohort year, evaluated the overall value of the program for themselves as 6.64, 6.52, and 6.61 and for Jefferson overall as 6.58, 6.65, and 6.65. Sponsors, for their part, when asked if they had seen “visible changes to date in the nature and quality of your sponsored participant’s leadership” responded, by year, on average 6, 5.63, and 5.82 on a scale running from inconsequential (1) to truly noteworthy (7). When asked “would you do it all again?”, sponsors across year responded on average 6.73, 6.5, and 6.6. A sample of stretch assignments appears in Table 1.
| Table 1: Examples of Stretch Assignments |
|
Participants and sponsors offered survey comments in keeping with the above reported numbers. A sample of them appear in Table 2.
| Table 2: Sample Participant and Sponsor Comments about Program Impact |
| Participant: “Leadership Academy [LA]made me a better person, not just a better leader”, “[LA] gave me the awareness of my own leadership abilities, deficiencies, and potential. It taught me the value of finding ways to make others better and trying to build confidence in those around you. It gave me enthusiasm”, “As a physician leader, I never learned the strategies to effect change—I feel better equipped and empowered now”, “[LA] gave me a systematic approach to manage change”, “Rather than a 3-4 year process, the center was open in just over one year”, “[LA] empowered me to effectively communicate and negotiate outside my division and department”, “[LA] provided a tremendous opportunity to network with colleagues from across the enterprise…Also pushed me to be more aggressive and results oriented”, “[LA] has had a powerful impact on me…I recognize myself as a leader here in a way that I never did. I have also built powerful alliances…I am not the same person I was before the program began…”
Sponsor:“[the participant’s] leadership persona has transformed, confidence, analytic approach and team building”, “Participant has shown a major change in focus, particularly his role as team member v. as an individual. Significant ‘Emotional Intelligence’ changes and personality insights”, “…more confident in her leadership style and in making contributions and sharing thoughts that are futuristic, change oriented, and optimistic,” “Incredible transformation over the year”, “Transformative impact on self-identification as a leader—and both the opportunities and responsibilities that implies…”, “Participant grew greatly during the year and will benefit her in the future”, “My participant is significantly better at modulating her response to situations which cause stress…”, “The program has broadened her scope and vision for sure. |
As for the above noted unanticipated measure, in year 3 and now in year 4, 29 of 64 sponsors or 45% of sponsors were either repeat sponsors, i.e., they had sponsored a participant previously, or were program alumni.
Discussion
The program clearly produced observable changes in participant leadership behavior across the competencies measured. Furthermore, participants and their sponsors evaluated the program as impactful and worthwhile, and the program provided the occasion to support projects befitting the stated program goals of improving organizational functioning amid dramatic growth, especially as experienced by patients. Hence, anyone seeking to achieve similar outcomes should consider carefully the program discussed in this article.
That said, as with any case study, the reader is left with questions of causation. These questions carry particular weight for anyone seeking to design and deliver a similar program with similar effect. For example, which program component had the most significant effect? How much did any aspect (e.g., emphasis on participative pedagogy and networking or explicit, public CEO support) contribute to the overall program impact, either in isolation or in combination? How much did the conscious and ongoing attempt to integrate the aspects of the program matter? Did the extensive sponsor involvement, while another example of best practice, play a noteworthy role in program impact? Would a similar program produce similar impact for a different type of cohort? To what extent did timing in the organization’s life, namely new CEO with a change and growth agenda, affect program impact? What is the program ROI and over what time span?
Jefferson Health
Jefferson Health is the brand for Thomas Jefferson University Hospitals Inc, a regional health system and academic medical center which currently has over 30,000 employees. It has grown rapidly over the life of the program under study, i.e., over the last 3 years. Currently, Jefferson Health includes or is scheduled to include the following facilities in greater Philadelphia: Thomas Jefferson University Hospital in Center City, Philadelphia, the Jefferson Hospital for Neuroscience, Methodist Hospital in South Philadelphia, Abington Memorial Hospital in the northern suburb of Abington, hospitals and various clinics of Aria Health in Northeast Philadelphia and Lower Bucks County, Kennedy Health facilities in southern New Jersey, and the Einstein Healthcare Network of the Delaware Valley along with 14 international affiliations. All told, Jefferson clinical personnel handle about 4.3m patient interactions a year.
Thomas Jefferson University’s roots go back to 1825. In July 2017, Thomas Jefferson University and Philadelphia University combined and created the newly named Jefferson University (9 colleges, 4 schools, and 160 undergraduate and graduate degrees). Additionally, Jefferson has over $122m in research funding.
References
- Lerman, C and Jameson, L. “Leadership Development in Medicine”, New England Journal of Medicine, 378;20: 1862-1863.
- Lucas, R, Goldman EF, Scott AR, Dandar V. “Leadership Development Programs at Academic Health Centers: Results of a National Survey”, Academic Medicine 2018; 93: 229-36.
- Boyatizis, RE. “Commentary on Ackley (2016): Updates on the ESCI as the Behavioral Level of Emotional Intelligence”, Consulting Psycology Journal: Practice and Research, 2016; v68, no.4: 287-293.
Amdurer, E Boyatzis, RE Saatcioglu, Smith ML, Taylor SN. “Long Term Impact of Emotional, Social, and Cognitive Intelligence Competencies and GMAT on Career and Life Satisfaction and Career Success”, Frontiers in Psychology, 2014, Dec, v5, article 1447: 1-15.
Do Providers Offer Medicaid Patients Different Services than Private Patients?
Karoline Mortensen, PhD, University of Miami Business School, Tianyan Hu, PhD, Merck, Aleeza Vitale, BS, George Washington University, Hanns Kuttner, AB, MA, Hudson Institute
Contact: Karoline Mortensen, kmortensen@bus.miami.edu
This research was supported internally by the Center for Health Management and Policy at the University of Miami Business School; the authors did not receive external funding for this research. Tianyan Hu completed the analyses and worked on the manuscript while she was an assistant professor at Florida International University.
Abstract
What is the message?
As entitlement programs are under pressure to demonstrate value and managed care penetration increases in Medicaid, gaps in knowledge exist about the characteristics of USC practices that serve Medicaid and privately insured patients. This study uses newly available data from the 2015 Medical Expenditure Panel Survey’s Medical Organization Survey, the first nationally representative data that include characteristics on individuals as well as the characteristics of the providers they use. Findings demonstrate that the usual source of care USC providers visited by adult, non-elderly Medicaid enrollees are just as likely as those used by the privately insured to be equipped with an Electronic Health/Medical Record system, provide same-day appointments, send patients reminders, and give physicians reports on clinical quality care, employ case managers, and have X-ray capacity on-site.
What is the evidence?
Analysis of data from a nationally representative survey of USC providers serving individuals who visited their USC in 2016 suggests that the organizational characteristics of providers do not differ significantly between those serving privately insured and Medicaid patients.
Submitted: May 18, 2018. Accepted after review: July 20, 2018.
Cite as: Karoline Mortensen, Tianyan Hu, Aleeza Vitale, Hanns Kuttner. 2018. Characteristics of Providers Serving Medicaid and Private Patients. Health Management Policy and Innovation, Volume 3, Issue 2.
Introduction
There is renewed focus on entitlement programs and the value they provide both taxpayers and their beneficiaries.1 There are concerns that the federal-state Medicaid program may provide inferior care and poor access to care relative to the access and quality enjoyed by the privately insured population. From a management perspective, it is difficult to address issues in Medicaid until there are data to demonstrate where gaps occur.
Medicaid enrollees have historically faced challenges in access to physicians, and these disparities regarding provider acceptance rate are well-documented.2-7 Medicaid patients are concentrated among a relatively small proportion of physicians.8 Median wait time for an outpatient office visit is longer for Medicaid enrollees (4.6 minutes) than for the privately insured (4.1 minutes), and Medicaid enrollees are 20 percent more likely to wait longer than 20 minutes.9 Payment generosity for Medicaid providers plays a significant role,10-13 and Medicaid enrollees face more barriers in securing an appointment with a provider than the privately insured.7,14,15 In-hospital mortality rates are lower for the privately insured than the Medicaid adult population.16 Primary care physicians in the highest tier of quality see more privately insured and fewer Medicaid patients than those in the lowest quality tier.17
However, there may be more parity than was previously thought in access, health services utilization, and delivery of care for the Medicaid population relative to the privately insured. Although overuse of low-value care is perceived to be common among Medicaid enrollees, rates of receipt of both low-value and high-value care are similar across publicly and privately insured patients.18 There is no evidence primary care physicians offer less care to Medicaid enrollees than the privately insured; in fact Medicaid patients received more diagnostic and treatment services than the privately insured.19
Furthermore, as the gap between state Medicaid-to-Medicare fee ratios narrowed, the acceptance of Medicaid patients by many providers was found to increase.6 Primary care appointment availability increased from 58.7 percent to 66.4 percent in 10 states between 2012 and 2014.20 In 2015, 64 percent of nurse practitioners and 59 percent of physicians stated that they had seen an increase in Medicaid patients or in new patients who were previously uninsured.21
Yet we still lack important information. Data limitations have made it difficult to compare the organizational and financial characteristics of the usual source of care providers accessed by Medicaid enrollees and the privately insured. Newly released data allows us to address this gap.
The Agency for Healthcare Research and Quality (AHRQ) has released the first nationally representative data set that links organizational characteristics of usual source of care providers with patients’ experiences.22 The existing literature is descriptive, examining differences in provider characteristics by race and insured/uninsured, but does not examine differences between the Medicaid and privately insured population.23 In this paper, we address this gap by examining the differences in characteristics of usual source of care providers accessed by Medicaid and privately insured respondents to the Medical Expenditure Panel Survey. Specifically, we analyze differences in provider organization characteristics, health information technology, practice case management and use of clinical quality data, and financial arrangements.
Health Information Technology. The prevalence of health information technology in health care is on the rise, partly as a result of incentives under the Affordable Care Act and HITECH Act, in effort to achieve greater care coordination, quality, and adaptability across care settings. In 2015, 87 percent of office-based physicians had adopted any electronic health record (EHR) system,24 up from 78 percent in 2013.25 The capabilities of these systems varied, as out 3 of 4 of these physicians (78 percent) adopted a certified EHR, and over 54 percent a “Basic EHR” system. This represents a significant increase of 66 percent in EHR utilization over the 11-year time frame.24 EHRs were present in practices serving 90 percent of patients who saw their usual source of care provider in 2015, with guidelines/screening reminders provided to 88 percent of patients.23 Furthermore, 78 percent of these EHR systems possessed secure messaging capabilities.23 Adoption of EHRs may be uneven, as large urban practices in Georgia are more likely to “Go Live” than similar rural environments, while Medicaid predominant providers are at a 47 percent higher risk of not achieving “Go Live” status in comparison to their private insurance counterparts.26
Case Management Clinical Quality. EHR capabilities (including clinical decision support, computerized physician order entry, and health information exchange) improve quality, reduce medical errors, and increase adherence to evidence-based clinical guidelines.28 Clinical information systems and patient scheduling systems are associated with adherence to best practices and greater total process quality.29
Financial arrangements. Physician remuneration method is strongly associated with technical quality of care.30 Almost 70 percent of physicians treating Medicaid patients indicate they receive variable compensation, with 67.7 percent of payment determined by productivity rather than quality and patient satisfaction.31 The concentration of Medicaid enrollees within a practice has implications for compensation. If 50 percent or more of a practice’s revenue is derived from Medicaid patients, physicians in that practice are 75 percent more likely to receive variable compensation than those with less than 5 percent Medicaid patients.31 Changes in physician income affect the likelihood that a physician may refuse to accept uninsured or Medicaid patients.32
Methods
Data and Samples The primary data source is the Medical Expenditure Panel Survey (MEPS) Medical Organizations Survey (MOS) data for 2015, fielded in 2016, maintained by the Agency for Healthcare Quality and Research (AHRQ). The data expands current Medical Provider Component of MEPS data by including information on the organizational characteristics of the practices of office-based care providers identified as a usual source of care in the Household Component (HC) and who were seen by the respondent in 2015. We further extract patient demographic and socioeconomic characteristics, as well as health conditions from 2015 MEPS consolidated file using the unique person identifier.
The Medical Organizations Survey is the first Federal survey to directly link practice characteristics with patient experiences.22 (The National Ambulatory Medical Care Survey asks physicians questions similar in nature, but does not link to nationally representative data and has a much shorter data collection window of visits that occur at a site within one randomly selected week.) The data are designed to provide nationally representative estimates of the characteristics of patients’ office-based usual source of care provider in 2015. The data are an internally consistent source of information on individuals’ characteristics, health care utilization and expenditures, and characteristics of the providers they use.33
The Medical Organizations analytic file contains 7,974 sample persons, associated with 4,216 unique responding practices (average of 1.7 sample persons per practice). Our analytic sample is a subset of this file that includes adults age 18-64 with either private insurance or Medicaid coverage for all of 2015, n=2,650.
Outcome Variables The outcome variables that we focus on in this paper are 1) provider organization characteristics; 2) practice implementation of health information technology; 3) practice case management and use of clinical quality data, and 4) financial arrangements. Tables 3 and 4 provide a detailed description of characteristics for each category.
Statistical Analyses We conduct descriptive analyses to examine differences in characteristics of primary care practices utilized by Medicaid and privately insured patients. Medicaid is defined by having received Medicaid insurance coverage for the entire year (fee-for-service or managed care), while private is an indicator for receipt of private health insurance coverage (via employer, exchanges, and other mechanisms) for the entire calendar year. We first compare summary statistics of patients’ characteristics as well as characteristics of providers that treat patients with Medicaid insurance and private insurance.
Patient characteristics include patients’ age categories (from 18 to 24; 25 to 34; 35 to 44; 45 to 54; and 55 to 64 years), sex, race and ethnicity categories (White non-Hispanic, African American non-Hispanic, Hispanic, and other race non-Hispanic), education level (below high school, beyond high school, 4-year college, beyond college), region of residence (Northeast, Midwest, South, and West regions), health status (excellent or very good, good, fair, or poor), whether patient has any chronic conditions, as well as whether patient ever had diabetes, asthma, high blood pressure, arthritis, emphysema, joint pain, heart disease and stroke.
Chi-squared tests assess statistical significance in the bivariate tabulations. We also analyze the association between provider characteristics for Medicaid and privately insured respondents using logistic regression to perform the estimation, controlling for respondents’ demographic and socioeconomic characteristics. In all analyses, we account for complex survey design including primary sampling unit, strata, and sampling weight in estimations. Analyses are conducted with Stata 14.1.
Results
Medicaid patients with a usual source of care provider that responded to the Medical Organizations Survey are more disadvantaged than private patients with a usual source of care on every dimension of disadvantage. There are significant differences in their demographic and socioeconomic characteristics, as well as health status (Table 1). More Medicaid patients are in younger age groups compared to private patients (18-24 group Medicaid vs private: 18.2 percent vs 8.8 percent, p=0.01; 25-34 group: 22.7 percent vs 14.6 percent, p=0.01); on the other end of the age range, fewer Medicaid patients are age 55-64, compared to private patients (18.7 percent vs 31.4 percent, p<0.001). More than 73 percent of Medicaid patients are female, compared to only 56.3 percent of private patients (p<0.001). The racial and ethnic compositions are different; 73.3 percent of private patients are non-Hispanic White, compared to only 43.0 percent of Medicaid patients (p<0.001). Medicaid patients are more likely to be non-Hispanic African American (21.6 percent vs 8.7 percent, p<0.001), or Hispanic (24.9 percent vs 9.5 percent, p<0.001) than the privately insured. Medicaid patients are also more likely to have lower than high school education (68.2 percent vs 30.3 percent, p<0.001), while private patients are more likely to be college educated (4.1 percent vs 23.9 percent, p<0.001), or have post graduate degrees (1.5 percent vs 16.3 percent, p<0.001).
More Medicaid patients perceive their physical health status as fair or poor (37.8 percent vs 10.5 percent, p<0.001) or good (33.8 percent vs 25.8 percent, p=0.02), instead of very good or excellent (28.4 percent vs 63.7 percent, p<0.001). Medicaid patients are also more likely to have any chronic conditions (68.4 percent vs 55.9 percent, p<0.001), specifically diabetes (16.7 percent vs 9.3 percent, p=0.01), asthma (16.8 percent vs 11.0 percent, p=0.04), high blood pressure (41.1 percent vs 32.4 percent, p=0.02), heart disease (4.4 percent vs 2.0 percent, p=0.03), and stroke (6.5 percent vs 2.8 percent, p=0.01). Respondents who saw their usual source of care in 2015 and are therefore in the MOS are older and also more likely to be female, white, and have chronic conditions than the general MEPS respondents (see Online Appendix Table 1 for demographic differences).
Organization Characteristics
Compared to private patients, Medicaid patients are more likely to be seen at nonprofit or government clinics (32.1 percent vs 26.1 percent, p<0.001) instead of independent practices (38.2 percent vs 51.2 percent, p=0.01). There are no statistically significant differences between the number of doctors or primary care providers at the practice seen by Medicaid and private patients. Fewer Medicaid patients see providers with no nurse practitioner or physician assistants (14.8 percent vs 24.7 percent, p=0.01). Medicaid patients are also more likely to visit multi-specialty group practices (48.4 percent vs 39.0 percent, p=0.02) and practices with more than one location (57.1 percent vs 40.9 percent, p<0.001).
Practice Implementation of Health Information Technology
There is no statistically significant difference between the percentage of practices with EHR/EMR system for Medicaid and private patients. Most of the practices seen by both types of patients are equipped with EHR/EMR systems (91.2 percent vs 93.2 percent, p=0.38). Over two thirds of patients with either Medicaid or private patients visit practices with EHR/EMR systems that send electronic reminders (68.5 percent vs 74.4 percent, p=0.11) or use secure electronic messages to communicate with patients (68.7 percent vs 75.3 percent, p=0.076).
Practice Case Management and Use of Clinical Quality Data
The results indicate that there are no statistically significant differences on any of the characteristics concerning case management and use of clinical quality data in the dimensions measured by the MOS between practices for Medicaid patients and those for private patients. Most practices provide same day appointments (91.3 percent vs 95.2 percent, p=0.10), send patients reminders (87.1 percent vs 88.3 percent, p=0.74), and give physicians reports on clinical quality care (76.5 percent vs 77.6 percent, p=0.77). Over half of practices employ case managers to coordinate patient care (55.6 percent vs 50.3 percent, p=0.22). Over a third of them also have an x-ray machine onsite (33.8 percent vs 40.6 percent, p=0.10).
Financial Arrangements
The types of patients also tend to cluster by type of practice. Significantly more Medicaid patients are seen by practices with greater than 50 percent Medicaid patients (47.1 percent vs 10.4 percent, p<0.001). Medicaid patients are also more likely to see practices that have capitated contracts (45.1 percent vs 33.3 percent, p=0.01) and pay physicians a base salary (52.2 percent vs 38.7 percent, p=0.005). By contrast, we do not observe significant differences with practices certified as a patient-centered medical home between Medicaid and private patients. We estimated each of these outcomes with logistic regression to control for demographic and socioeconomic status, with similar results (see Online Appendix Table 2).
Limitations
Our study has several limitations. Data are only available for respondents who saw their usual source of care in 2015, so these results are only representative of Medicaid and privately insured patients who accessed their usual source of care. This is the first year of the MOS, so there are no prior data for comparative analysis. Knowledge of practice capabilities varies depending on the staff respondent at the provider practice site and AHRQ does not impute data in this survey, so some questions generate high “don’t know/refused” responses.
Discussion
Our results show that while health status and demographic characteristics between Medicaid patients and their privately insured counterparts differ, fewer disparities are identified in the organizational characteristics and structural quality of care of providers between the two groups. Although Medicaid patients are more likely to be seen at nonprofit or government facilities, the number of doctors or primary care providers at the practice seen by Medicaid and private patients remains similar. A large and similar share of both Medicaid and privately insured patients usually visit practices that utilize EHR/EMR systems and over two thirds of patients, regardless of status, visit practices that send electronic reminders. Case and clinical quality management, additionally, does not seem to be impacted by Medicaid or private insurance status.
Nonetheless, more Medicaid patients are seen by practices in which Medicaid patients are a significant part of their patient base. This is consistent with the previous literature.8
Our results have important implications for future policy emphasis. While there is seemingly more parity regarding quality of care among Medicaid and private pay patients, health status still varies between the two groups. Despite the differences in health status, few disparities are seen in several measures of structural quality of care and services offered between these two patient groups. While initial concerns regarding the federal-state Medicaid program’s care and access capabilities are warranted, our data suggests that the dimensions of structural quality of care examined in this analysis are similar across the Medicaid and privately insured patient population.
Policy Implications
To our knowledge, this is the first study to use nationally representative data to compare the organizational characteristics of providers treating Medicaid and private pay patients. Perhaps surprising, we find that the characteristics of these practices are quite similar. The inferior access and capability arguments among Medicaid providers could soon become relics of the past.
The United States has been experiencing a significant transformation in the delivery of publicly financed health insurance, with the majority of enrollees (approaching 80 percent) in the Medicaid program in private insurance plans funded by the government.34 Managed care plans achieve savings for Medicaid through the government’s ability to negotiate lower prices with health plans rather than impacting the actual practice of Medicaid providers.35 These structural changes could explain the similarities in practice characteristics.
Future work should further explore the organizational and patient characteristics in the MEPS MOS survey data, as they relate to different health outcomes in the Medicaid and privately insured populations. While the rapid transition of EHR adoption has resulted in equity in practices visited by Medicaid and private patients, whether this parity in adoption leads to improved outcomes is still to be determined.
Table 1: Demographic and Socioeconomic Characteristics by Insurance Coverage
|
Insurance Type |
||||||||
| Variable | Private (%) | Medicaid (%) | P-value | |||||
| Age | ||||||||
| 18-24 | 8.8 | 18.2 | 0.01 | |||||
| 25-34 | 14.6 | 22.7 | 0.01 | |||||
| 35-44 | 19.1 | 18.8 | 0.91 | |||||
| 45-54 | 26.2 | 21.5 | 0.19 | |||||
| 55-64 | 31.4 | 18.7 | 0.01 | |||||
| Sex | ||||||||
| Male | 43.7 | 26.6 | 0.01 | |||||
| Female | 56.3 | 73.4 | 0.01 | |||||
| Race/Ethnicity | ||||||||
| Non-Hispanic white | 73.3 | 43.0 | 0.01 | |||||
| Non-Hispanic black | 8.7 | 21.6 | 0.01 | |||||
| Other | 8.5 | 10.5 | 0.55 | |||||
| Hispanic | 9.5 | 24.9 | 0.01 | |||||
| Education | ||||||||
| DK | 0.1 | 1.0 | ||||||
| 9-12 years | 30.3 | 68.2 | 0.01 | |||||
| Beyond high school | 29.4 | 25.2 | 0.22 | |||||
| 4-year college | 23.9 | 4.1 | 0.01 | |||||
| Master or higher | 16.3 | 1.5 | 0.01 | |||||
| Region | ||||||||
| Northeast | 20.7 | 25.7 | 0.27 | |||||
| Midwest | 23.5 | 19.4 | 0.24 | |||||
| South | 34.2 | 26.2 | 0.07 | |||||
| West | 21.7 | 28.7 | 0.14 | |||||
| Perceived Health Status | ||||||||
| DK | 0.0 | 0.0 | ||||||
| Very good/excellent | 63.7 | 28.4 | 0.01 | |||||
| Good | 25.8 | 33.8 | 0.02 | |||||
| Fair/poor | 10.5 | 37.8 | 0.01 | |||||
| Chronic Condition | ||||||||
| No | 44.1 | 31.6 | 0.01 | |||||
| Yes | 55.9 | 68.4 | 0.01 | |||||
Notes: Author’s analysis of the 2015 Medical Expenditure Panel Survey (MEPS) Medical Organizations Survey (MOS) data. Data are only for respondents to the MEPS who reported visiting their usual source of care in 2015, n=7,952. DK=respondent at provider’s office didn’t know this information.
Table 2: Differences in Organizational Characteristics and Types of Practices by Insurance
| Type of Practice | Private (%) | Medicaid (%) | P Value | |
| DK/REFUSED | 3.7 | 1.7 | ||
| Independent practice | 51.2 | 38.2 | 0.01 | |
| Physician network hospital owned | 26.1 | 19.6 | 0.16 | |
| Nonprofit or government clinic | 10.8 | 32.1 | 0.01 | |
| Practice owned academic medical center | 3.0 | 2.6 | 0.78 | |
| HMO | 1.5 | 0.3 | 0.05 | |
| Corporation owned | 2.9 | 3.7 | 0.54 | |
| Other | 0.9 | 1.9 | 0.35 | |
| Number of Physicians | ||||
| DK/REFUSED | 5.0 | 5.6 | ||
| 0 | 0.6 | 1.3 | 0.53 | |
| 1 | 19.3 | 18.2 | 0.72 | |
| 2-3 | 25.2 | 24.0 | 0.77 | |
| 4-10 | 27.0 | 21.4 | 0.13 | |
| 11-50 | 17.9 | 25.1 | 0.10 | |
| 51-100 | 2.5 | 1.6 | 0.28 | |
| 101-249 | 0.8 | 1.3 | 0.63 | |
| 250 | 1.7 | 1.6 | 0.87 | |
| Number of PCP | ||||
| DK/REFUSED | 6.0 | 7.4 | ||
| 0 | 4.4 | 7.7 | 0.29 | |
| 1 | 19.5 | 20.0 | 0.87 | |
| 2-3 | 25.9 | 22.2 | 0.31 | |
| 4-10 | 27.4 | 21.2 | 0.06 | |
| 11-50 | 15.0 | 20.0 | 0.19 | |
| 51-100 | 1.9 | 1.5 | 0.62 | |
| Number of NP and PA | ||||
| DK/REFUSED | 5.8 | 7.3 | ||
| 0 | 24.7 | 14.8 | 0.01 | |
| 1 | 20.7 | 20.9 | 0.95 | |
| 2-3 | 24.7 | 24.6 | 0.97 | |
| 4-10 | 19.7 | 23.6 | 0.28 | |
| 11-49 | 3.6 | 7.5 | 0.06 | |
| 50 | 0.9 | 1.3 | 0.35 | |
| Is the Practice a Multi-Specialty Group Practice? | ||||
| DK/REFUSED | 0.7 | 2.3 | ||
| Yes | 39.0 | 48.4 | 0.02 | |
| No | 60.2 | 49.3 | ||
| Does the Practice Have More Than One Location? | ||||
| DK/REFUSED | 0.0 | 0.2 | ||
| YES | 40.9 | 57.1 | 0.01 | |
| NO | 59.1 | 42.7 | ||
Notes: Author’s analysis of the MEPS MOS database. HMO is health maintenance organization. PCP is primary care provider. NP is nurse practitioner. PA is physician assistant. DK/REFUSED is respondent for provider practice didn’t know/refused.
Table 3: Electronic Medical Record Usage and Features
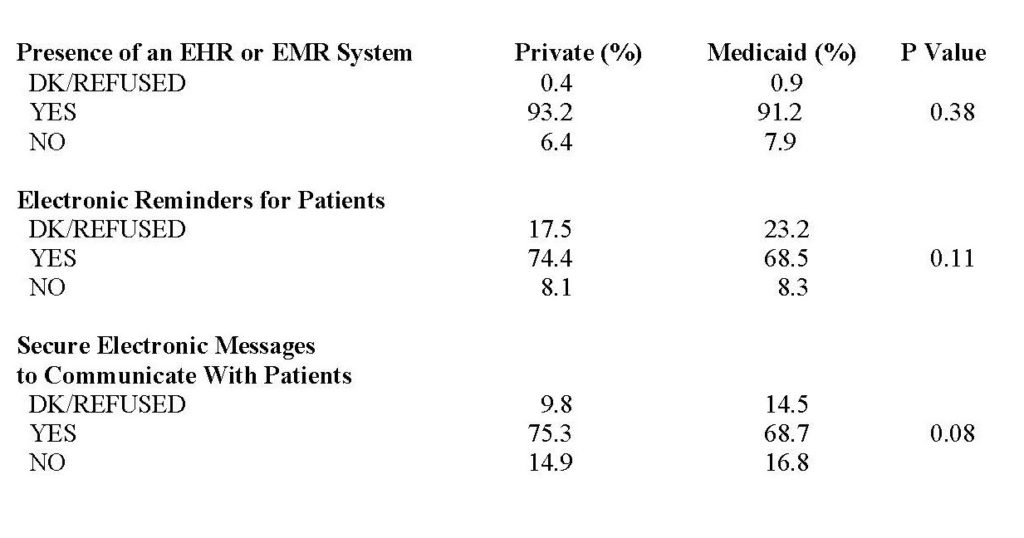
Notes: Author’s analysis of the MEPS MOS database. EHR is electronic health record. EMR is electronic medical record. Utilization is compared across Medicaid and private pay patients.
Table 4: Differences in Practice Case Management & Use of Clinical Quality Data by Insurance Status
| Insurance Status | ||||
| Provide Same Day Appointments? Private (%) | Medicaid (%) | P Value | ||
| DK/REFUSED | 0.7 | 2.7 | ||
| Yes | 95.2 | 91.3 | 0.10 | |
| No | 4.2 | 6.1 | ||
| Send Patients Reminders? | ||||
| DK/REFUSED | 2.0 | 2.4 | ||
| Yes | 88.3 | 87.1 | 0.73 | |
| No | 9.8 | 10.5 | ||
| Have An X-ray Machine On Site? | ||||
| DK/REFUSED | 1.6 | 0.2 | ||
| Yes | 40.6 | 33.8 | 0.10 | |
| No | 57.8 | 65.9 | ||
| Give Reports To Physicians
On Clinical QOC? |
||||
| DK/REFUSED | 13.2 | 14.7 | ||
| Yes | 77.6 | 76.5 | 0.77 | |
| No | 9.3 | 8.8 | ||
| Employ Case Managers To
Coordinate Patient Care? |
||||
| DK/REFUSED | 6.7 | 4.7 | ||
| Yes | 50.3 | 55.6 | 0.22 | |
| No | 43.1 | 39.7 | ||
| Contact The Patient Within 48
Hours of Discharge From Hospital? |
||||
| DK/REFUSED | 7.0 | 9.1 | ||
| Yes | 68.9 | 66.6 | 0.59 | |
| No | 24.2 | 24.3 | ||
Notes: Authors’ analysis of the MEPS MOS database. QOC is quality of care.
Limited Public Support for Team-Based Care Models – Survey Results
Rachel A. Hadler, MD1*, Julia F. Lynch, PhD2*, Julia Berenson, MSc3, Lee A. Fleisher, MD1
Contact: Rachel A. Hadler, Rachel.hadler@uphs.upenn.edu
* These authors contributed equally to this work.
Acknowledgements: This project was partially funded by a 2013 Pilot Grant from the Leonard Davis Institute for Health Economics at the University of Pennsylvania. Findings from this study were previously presented by R. Hadler and J. Berenson at Academy Health in Boston in June, 2016.
Abstract
What is the message?
We evaluated perceptions of the desirability and quality of care provided by nurse practitioners and physicians, as well as the acceptability of different trade-offs allowing direct access to physician providers. Significant segments of the public perceived physician-provided care as preferable to team-based care. Respondents more likely to support ungated access to physicians were nonwhite, experiencing financial hardship, older, and/or identified as Republican. Similar characteristics predicted perceptions that seeing a nurse practitioner resulted in worse care and willingness to pay to guarantee direct access to physicians without seeing an NP first. There was little political consensus on acceptability of specific trade-offs that might facilitate increased physician access.
What is the evidence?
An internet-based survey of 3650 U.S. citizens exposed to sample care scenarios with nurse practitioners or physicians as primary provider across multiple care settings and insurance types and asked to evaluate quality and desirability of care.
Submitted: May 18, 2018; accepted after review: July 20, 2018
Cite as: Rachel A. Hadler, Julia F. Lynch, Julia Berenson, Lee A. Fleisher. 2018. Limited Public Support for Team-Based Care Models: Survey Results. Health Management Policy and Innovation, Volume 3, Issue 2.
Introduction
The past decade has seen significant change in the federal approach to health care delivery in the United States. The passage of the Affordable Care Act (ACA) in 2010 was hailed by liberals as an important step towards universalizing access to care, but scorned by conservatives as costly and emblematic of government overreach.[1] In spite of ongoing debate and generally negative perceptions in the polls,[2] [3] [4] coverage under the ACA has continued to expand over the seven years since its enactment,[5] generating an increased need for healthcare providers[6]. In early discussions regarding expected workforce shortages, the team-based care model, which involves collaborative delivery of care by physician and non-physician providers such as nurse practitioners (NPs), was hailed as a means of expanding the healthcare workforce[7] [8] and allowing insurance plans to meet requirements for minimum guaranteed benefits while containing costs.[9] [10] [11] [12] [13]
Existing research indicates that patients enjoy similar outcomes whether seen by a nurse practitioner or physician, [14] [15] suggesting that non-physician providers could address the shortage of primary care doctors as long as appropriate systems for escalation were in place. [16] [17] While studies have found that the public is generally enthusiastic about nurse practitioners as primary care and outpatient specialist providers,[18][19] less is known about the public’s understanding or acceptance of team-based care models in non-routine settings, and there is no research on how these attitudes are related to political partisanship, a key predictor of healthcare policy attitudes.
Existing research on consumer attitudes towards tiered access to care based on hospital or provider characteristics suggests that the public is wary but not unequivocally opposed to such a model if it is accompanied by significant gains in quality.[20] [21] Given this context, we chose to examine public attitudes toward the quality and desirability of a team-based care model in which nurse practitioners act as primary providers with physician backup. Our goal in fielding this nationally representative survey was to assess public acceptance of rationed access to physicians by insurance providers across several distinct clinical contexts.
Methods
Study design
We used an experimental design embedded in a survey (Appendix) to estimate the effect on respondents’ support for limiting access to physician providers based on the type of insurance held by a fictitious patient and the setting in which care was sought. This type of experimental design has been used extensively in health policy research to circumvent some of the limitations of traditional cross-sectional surveys and to clarify the relationships identified by classic survey work.[22] [23] [24] Heart disease was selected as a pathology of interest based on existing precedents for advanced practice provider (APP)-driven care in the outpatient environment.[25] [26] [27]
The survey was developed in collaboration with colleagues in healthcare and policy, and was pre-tested for clarity on a convenience sample of respondents using Survey Monkey. It was fielded in August 2014 by YouGov, an Internet-based market research firm that also fields scholarly surveys. Respondents were American citizens over 18 years of age enrolled in YouGov’s opt-in Internet panel.
After responding to several questions assessing pre-treatment attitudes towards healthcare and policy, participants were exposed to a brief informational module explaining the degree of federal subsidization for three levels of insurance under the ACA, and tested to ensure that the relevant information was salient. They were then presented with one of nine possible vignettes describing a male patient who has heart failure (HF) and whose insurance “will only cover the costs for him to see a doctor if a nurse practitioner could not provide the same care.” Two aspects of the patient’s care vignette were randomly manipulated for each respondent: (1) health insurance type and (2) care setting. (Figure 1)
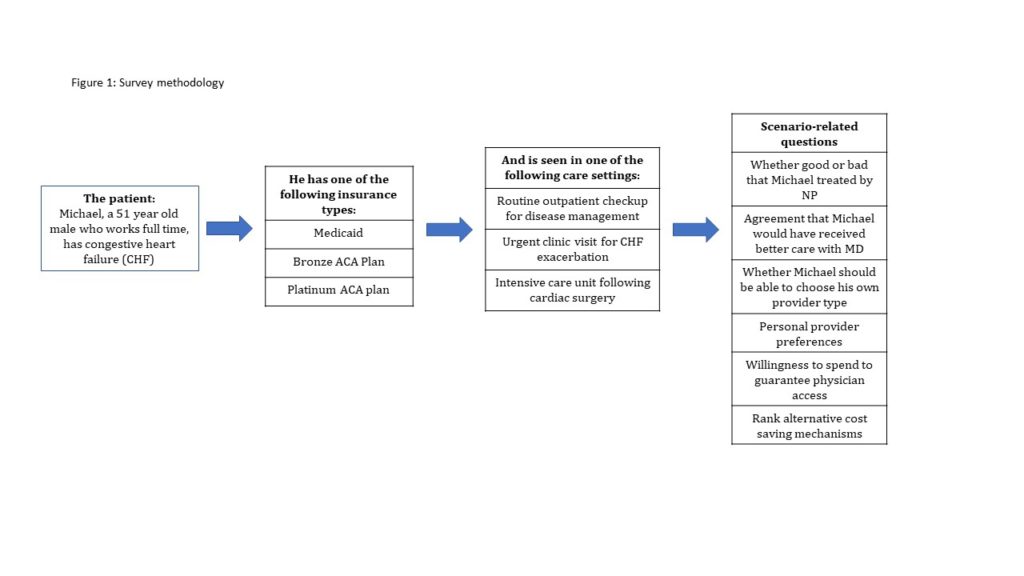
Following the vignette, respondents were asked to evaluate the quality and cost of care received from the assigned provider before answering questions about their provider preferences and willingness to pay to guarantee direct access to a physician. Respondents then ranked a variety of alternatives to limiting direct access to physicians as means of reducing/ stabilizing healthcare costs: 1) increased insurance premiums; 2) longer wait times; 3) increased out of pocket costs for medication; 4) increased out of pocket expenses for office visits; 5) reduced subsidies for low income populations; and 6) increased taxes to increase resources for health care. Respondents were also asked to provide demographic data.
Statistical Methods
Sample weights provided by YouGov were used to correct for observable imbalances between responders and nonresponders, and to weight individuals to a nationally representative sample. Initial descriptive analysis involved comparing mean responses for opinion questions across all nine treatment groups. In keeping with conventions in attitudinal research, Likert scales were treated as linear.
Linear regressions were performed to evaluate the mean effect of the care setting and insurance type manipulations among subgroups of survey respondents. Multinomial logit models were used to analyze how cost control options were affected by the insurance and care setting treatments. Ordinal least squares (OLS) models were used to predict the relationship between the insurance treatment conditions and opinions about provider choice, as well as to predict the relationship between treatment conditions and opinions about the desirability of specific policy options which would allow increase physician access. All statistical analyses were performed using STATA (V14, College Station, TX).
Results
Our survey had a within-panel response rate (AAPOR 4) of 55% (of 8255 YouGov panelists invited, 4357 elected to participate). Non-responders were statistically indistinguishable from responders in terms of household income and political party identification, but were more likely than respondents to be male, non-white, and have lower educational attainment. From these respondents, the 3,650 respondents included in the final sample were weighted to a nationally representative sampling frame matched on voter registration status and turnout, interest in politics and party identification, age, gender, race/ethnicity, educational attainment and ideology.
The survey indicated a substantial preference for physicians over non-physicians, with several factors reinforcing the preference. A large majority of respondents (79%) supported insurance companies allowing patients having direct access to physician providers regardless of care setting or insurance type (Table 1). Nonwhite respondents, those experiencing financial hardship, older respondents, and Republicans were more likely to report a personal preference for being seen by a physician provider.
Table 1: Support for ungated access to physician providers by care setting and insurance treatments
| Care Setting Treatment | Insurance Condition Treatment | ||||||
| Total sample (%) | Outpatient
Routine (%) |
Outpatient Acute (%) | Inpatient (%) | Medicaid (%) | Bronze (%) | Platinum (%) | |
| Michael should be able to choose to see a physician | |||||||
| Disagree Strongly | 5.0 | 4.1 | 6.4 | 4.5 | 6.5 | 4.7 | 3.8 |
| Disagree somewhat | 18.0 | 18.4 | 16.9 | 18.8 | 22.2 | 18.1 | 13.8 |
| Agree somewhat | 40.6 | 40.5 | 40.0 | 41.2 | 40.6 | 42.8 | 38.4 |
| Agree Strongly | 36.4 | 36.9 | 36.7 | 35.6 | 30.6 | 34.5 | 44.0 |
Financial hardship, fair or poor self-assessed health status, and older age were predictive of willingness to pay an additional fee for guaranteed access to a physician (nonwhite, uninsured, age and Republican), and of perceiving that a nurse practitioner would provide worse care for the fictitious patient than would a physician. Respondents’ belief that physician care would be preferable in this scenario, their personal preference to be seen by an MD under similar circumstances, and the amount they would be willing to pay to ensure ungated access to a physician were all strong predictors of support for the vignette protagonist having ungated access to physician providers.
Political ideology strongly conditioned the effect of the insurance treatment on opinions regarding the desirability of ungated provider choice (p<0.05; Table 2). Although both liberals and conservatives exposed to the Platinum insurance treatment supported ungated access to physicians, conservatives exposed to the Medicaid insurance treatment were significantly less likely than liberals to agree that patients like the vignette protagonist should have provider choice. Similar patterns emerged across surrogates for political partisanship such as conservatism and low egalitarianism score.
Table 2: OLS regression coefficients (p-values in parenthesis) for models predicting support for ungated access to physician providers
| A | B | C | D | E | |
| Insurance Treatment | |||||
| Platinum | 0.1029 (0.022) | 0.1002 (0.023) | 0.9787 (0.026) | 0.1005 (0.022) | 0.1034 (0.135) |
| Medicaid | -0.1476 (0.002) | -0.1465 (0.001) | -0.1600 (0.000) | -0.1581 (0.000) | -0.2248 (0.001) |
| Demographics | |||||
| Nonwhite | 0.03964 (0.371) | 0.008418 (0.849) | -0.03100 (0.491) | -0.02664 (0.551) | |
| Under 400% poverty | 0.04852 (0.244) | 0.03680 (0.375) | 0.03395 (0.412) | 0.03150 (0.444) | |
| Financial hardship | 0.07762 (0.000) | 0.05651 (0.008) | 0.05819 (0.006) | 0.06374 (0.003) | |
| Some/ 2-year college | -0.04693 (0.305) | -0.03483 (0.444) | -0.03509 (0.441) | -0.03207 (0.475) | |
| 4-year college/ post-graduate work | -0.1667 (0.000) | -0.1327 (0.006) | -0.1368 (0.005) | -0.1386 (0.004) | |
| Fair/ poor health status | -0.02477 (0.624) | -0.03059 (0.540) | -0.03504 (0.479) | -0.04206 (0.386) | |
| Uninsured | -0.01409 (0.816) | 0.05852 (0.325) | 0.05408 (0.365) | 0.04512 (0.446) | |
| Currently insured under Medicaid | 0.08744 (0.185) | 0.09591 (0.147) | 0.08630 (0.193) | 0.07812 (0.229) | |
| Currently insured under Medicare | 0.05527 (0.301) | 0.09761 (0.069) | 0.09203 (0.087) | 0.09029 (0.090) | |
| History of heart attack | 0.006755 (0.873) | 0.1989 (0.630) | 0.02143 (0.603) | 0.02177 (0.594) | |
| Age | 0.01954 (0.002) | 0.01868 (0.002) | 0.01816 (0.003) | 0.01930 (0.001) | |
| Age-squared | 0.0002053 (0.002) | 0.000213 (0.001) | 0.000205 (0.001) | 0.0002161 (0.000) | |
| Personal preferences | |||||
| Personally prefer to see physician | 0.1581 (0.000) | 0.1575 (0.000) | 0.1569 (0.000) | ||
| Amount willing to pay | 0.02660 (0.001) | 0.02745 (0.000) | 0.0273 (0.000) | ||
| Bad for Michael to see NP | 0.06015 (0.006) | 0.06170 (0.005) | 0.05496 (0.011) | ||
| Political party | |||||
| Democrat | 0.04448 (0.311) | 0.02911 (0.695) | |||
| Republican | -0.7792 (0.077) | -0.1631 (0.019) | |||
| Interactions | |||||
| Platinum/ Democrat | -0.1673 (0.107) | ||||
| Platinum/ Republican | -0.16305 (0.019) | ||||
| Medicaid/ Democrat | 0.1948 (0.063) | ||||
| Medicaid/ Republican | 0.01444 (0.889) | ||||
| R-Squared | 0.0146 | 0.0439 | 0.1273 | 0.1298 | 0.1418 |
We found widespread agreement that ungated access to physician providers was desirable. However, few respondents, regardless of political affiliation, expressed willingness to sacrifice other aspects of value in order to finance ungated physician-level care for all patients. Table 3 reports the share of respondents endorsing policy changes such as higher premiums, longer wait times, or reduced subsidies to allow ungated access. Fewer than one in ten respondents definitively endorsed any of the policy solutions, and no more than one in four was willing to voice even qualified acceptance of the options listed.
Table 3: Share of respondents endorsing policy options to free up resources for ungated access to physician providers
| Policy Option | Definitely Good | Possibly Good | Possibly Bad | Definitely Bad |
| Increase insurance premiums for all patients | 5.6 | 18.6 | 33.2 | 42.7 |
| Have all patients wait longer to see a specialist for nonemergent visits | 4.6 | 25.0 | 37.4 | 33.0 |
| Increase copays for medications | 3.2 | 13.7 | 34.9 | 48.2 |
| Increase copays for visits to medical office | 3.2 | 18.2 | 34.9 | 43.6 |
| Cut back subsidies for health insurance for people with low incomes | 8.5 | 22.6 | 29.6 | 39.3 |
| Raise taxes | 6.99 | 23.3 | 25.9 | 43.9 |
When faced with a forced choice, over half of respondents favored either raising taxes or lowering subsidies in order to ensure ungated access to physicians. The choice of these options was highly partisan (Table 4): 46% of liberals and only 8% of conservatives endorsed raising taxes as the most desirable option, whereas 40% of conservatives and only 12.5% of liberals supported reducing insurance subsidies for low-income people.
Table 4: Share of respondents endorsing first and second choice policy options, by political ideology
| Political Ideology | ||||
| Total Sample (%) | Conservative (%) | Moderate (%) | Liberal (%) | |
| First policy choice | ||||
| Reduce subsidies for health insurance for people with low incomes | 25.9 | 39.8 | 23.4 | 12.5 |
| Raise taxes | 25.5 | 8.4 | 26 | 45.6 |
| Second policy choice | ||||
| Reduce subsidies for health insurance for people with low incomes | 8.6 | 9.7 | 8.8 | 7 |
| Raise taxes | 8.5 | 4.6 | 10 | 11.1 |
Discussion
Despite widespread enthusiasm in the health policy community for team-based care models,9 the American public remains skeptical about insurance restrictions that would limit direct access to physicians. The public’s unequivocal endorsement of unfettered provider choice is in line with other studies suggesting that despite incentives encouraging use of low-cost, high-quality providers,[28] [29] uptake has been limited. Factors influencing these consumer choices may include perceptions that lower cost providers provide lower quality care[30] as well as loyalty to specific providers[31][32] and trusted referral sources.21
Our research also reveals a stark political divide in attitudes toward cost savings in healthcare. While liberals and conservatives agree on the undesirability of the gated access to physician-level providers central to team-based care for those with insurance plans with no federal subsidy, they disagree about whether patients with subsidized plans should have unrestricted access to physician care, and about how to pay for this guaranteed access to physicians.
Many policymakers see an important role for team-based care. Team-based care has been associated with reduced readmission rates;30 numerous evaluations of care provided by nurse practitioners in primary care settings have shown higher patient satisfaction rates with similar outcomes and costs in comparison to physicians. [33], [34] A 2001 Institute of Medicine Report called for an enhanced role of team-based care in future healthcare.[35] In spite of this, our findings suggest that many Americans, particularly those most likely to be impacted by such a policy change, continue to perceive physician-driven care as more desirable.
This combination of enthusiasm among policy elites and skepticism among the public is reminiscent of the debates over the introduction of Health Management Organizations (HMO) in the 1980s and 1990s. The poor outcomes of most HMO initiatives should serve as a reminder that unfavorable public opinion can derail even policies that receive widespread political endorsement and public utilization. If team-based care models are to avoid the fate of HMOs, health policy makers must educate the public about their cost effectiveness and quality, and find ways to overcome partisan divides underlying healthcare attitudes.
The nature of our sample imposes some limits on the generalizability of our findings. YouGov’s online panel, from which our sample was drawn, is weighted to match the national population in terms of gender, age, race, education, political party identification, ideology, and interest, voter registration and turnout. Survey weights further correct for any random imbalances with respect to the national population. The uninsured and Medicare recipients are nevertheless somewhat overrepresented in our survey’s weighted sample as compared to the 2014 Current Population Survey (CPS),[36] whereas Medicaid patients are underrepresented. Although our analysis controls for insurance status, this feature of the sample should be taken into account when extrapolating our findings to a national frame.
Although the methodology has been used in other health policy work[23] [24], the central questions in our survey are new and unvalidated. Our survey instrument framed the restrictions on physician access in the context of insurance, rather than as a change induced by incentives in the ACA or at the initiative of medical practice groups. In fact, all of these actors have pushed in the direction of more team-based care. Given the hostility of many Americans to insurance companies, this framing may result in a more negative view among respondents toward the use of NPs as first-line providers. Finally, our survey assesses respondents’ opinions in response to written clinical vignettes, which may not accurately represent their behavior in real-world care-seeking situations.
This study suggests that policy makers interested in reducing health care costs through gated access programs have three choices: (1) to maintain the status quo, whereby access to physician providers is rationed according to ability to pay, a solution that is objectionable to many members of the public; (2) to forge a consensus on policy measures that could be undertaken to finance more widespread access to physicians; or (3) to educate the public about the benefits of team-based care. We believe that some combination of the three is probably an optimal compromise solution, given the wide divergence between political groups on the desirability of other cost-saving measures, differences of opinion about the desirability of tiering access to physicians by insurance, and the current gap between expert and lay beliefs.
Appendix
Tiering-Hadler-Appendix-Survey Instrument
References
- Pew Research Center. More Americans disapprove than approve of health care law. 2016 Apr 27. [cited 2016 Sept 28]. In Pew Research Center: U.S. Politics and Policy [Internet]. Philadelphia (PA): Pew Charitable Trust. Available from: http://www.people-press.org/2016/04/27/more-americans-disapprove-than-approve-of-health-care-law/.
- Blendon RJ and Benson JM. Voters and the Affordable Care Act in the 2014 Election. New England Journal of Medicine 2014;371:1-7.
- Jones, Jeffrey M. Americans’ views of healthcare law improve. 2015 July 10. [Cited 2016 September 28]. In Gallup News: Politics [Internet]. Washington, D.C.: Gallup, Inc. Available from: http://www.gallup.com/poll/184079/americans-views-healthcare-law-improve.aspx.
- Kaiser Family Foundation. Kaiser Health Tracking Poll: the public’s views on the ACA. 2016 Sept 27. [Cited 2016 Sept 27]. In KFF.org [Internet], Menlo Park (CA): Kaiser Family Foundation. Available from: http://kff.org/interactive/kaiser-health-tracking-poll-the-publics-views-on-the-aca/#?response=Favorable–Unfavorable&aRange=twoYear.
- McMorrow S, Polsky, D. Issue Brief: Insurance coverage and access to care under the Affordable Care Act. 2016 Dec 8. [Cited 2017 Aug 17]. LDI ACA Impact Series [Internet]. Philadelphia (PA), Leonard Davis Institute. Available from: https://ldi.upenn.edu/brief/insurance-coverage-and-access-care-under-affordable-care-act).
- Heisler EJ. Physician supply and the Affordable Care Act. Washington, DC: Congressional Research Service; 2013 Jan. Report No. R42029. Available from https://pdfs.semanticscholar.org/0630/1e4333be895712830e9c5f0f1dfd8a8fa2f5.pdf.
- Auerbach DI, Chen PG, Friedberg MW, Reid R, Lau C, Buerhaus PI, Mehrotra A. Nurse-managed health centers and patient-centered medical homes could mitigate expected primary care physician shortage. Health Affairs. 2013;32:1933-1941.
- Green, LV, Savin S, Lu Y. Primary care physician shortages could be eliminated through use of teams, nonphysicians, and electronic communication. Health Affairs. 2013;32:11-19.
- Essential Health Benefits Requirements Act of 2010. Pub. L. 111-148, 124 Stat.782 (Mar 23, 2010).
- Public Health Service Act of 1944, 42 U.S.C. Ch 6(a),§ 300gg (2010).
- U.S. Department of Health and Human Services. Insurance Standards Bulletin Series–Extension of Transitional Policy through October 1, 2016. Available from: http://www.cms.gov/CCIIO/Resources/Regulations- and-Guidance/Downloads/transition-to-compliant-policies-03-06-2015.pdf.
- Department of Health and Human Services. Patient Protection and Affordable Care Act; Standards Related to Essential Health Benefits, Actuarial Value, and Accreditation. Federal Register 2013;78:12834-12872.
- Giovannelli J, Lucia KW, and Corlette S. Implementing the Affordable Care Act: Revisiting the ACA’s Essential Health Benefits Requirements. Commonwealth Fund 2014; 1783:1-12.
- Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. British Medical Journal. 2002;324: 819–23.
- Naylor MD and Kurtzman ET. The Role Of Nurse Practitioners In Reinventing Primary Care. Health Affairs. 2010;29:893-899
- Margolius D, Bodenheimer T. Transforming Primary Care: From Past Practice To The Practice Of The Future. Health Affairs. 2010;29(5):779-84
- Grumbach K and Bodenheimer T. Can health care teams improve primary care practice? Journal of the American Medical Association. 2004;291:1246–51.
- Dill MJ, Pankow S, Erikson C, Shipman S. Survey Shows Consumers Open To A Greater Role For Physician Assistants And Nurse Practitioners. Health Affairs. 2013;32:1135-1142.
- Brown DJ. Consumer perspectives on nurse practitioners and independent practice. Journal of the American Academy of Nurse Practitioners. 2007;19:523-529.
- Harris KM. Can high quality overcome consumer resistance to restricted provider access? Evidence from a health plan choice experiment. Health Services Research. 2002;37:551-71.
- Sinaiko AD. How do quality information and cost affect patient choice of provider in a tiered network setting? Results from a survey. Health Services Research. 2011;46:437-56.
- Gaines BJ and Kuklinski JH. The logic of the survey experiment reexamined. Political Analysis. 2007;15:1-20.
- Gollust SE, Lynch J. Who deserves health care? The effects of causal attributions and group cues on public attitudes about responsibility for health care costs. Journal of Health Politics, Policy and Law. 2011;36:1061-1095.
- Tesler M. The spillover of racialization into health care: how President Obama polarized public opinion by racial attitudes and race. American Journal of Political Science 2012;56:690-704.
- David D, Brittling L, Dalton K. Cardiac acute care nurse practitioner and 30-day readmission. Journal of Cardiovascular Nursing. 2015;30:248-255.
- Hall MH, Esposito RA, Pekmezaris R, Lesser M, Moravick D, Jahn L, Blenderman R, Akerman M, Nouryan CN, Hartman AR. Cardiac surgery nurse practitioner home visits prevent coronary artery bypass graft readmissions. Annals of Thoracic Surgery. 2014;97:1488-1493.
- Lowery J, Hopp F, Subramanian U, Wiitala W, Welsh DE, Larkin A, Stemmer K, Vaitkevicius P. Evaluation of a nurse practitioner disease management model for chronic heart failure: a multi-site implementation study. Congestive Heart Failure. 2012;18:64-71.
- Brennan TA, Spettell CM, Fernandes J, Downey RL, Carrara LM. Do managed care plans’ tiered networks lead to inequities in care for minority patients? Health Affairs. 2008;27:1160-116.
- Tackett S, Stelzner C, McGlynn E, Mehrotra A. The impact of health plan physician-tiering on access to care. Journal of General Internal Medicine 2011;26:440-445.
- Mehrotra A, Hussey PS, Milstein A, Hibbard JH. Consumers’ and providers’ responses to public cost reports, and how to raise the likelihood of achieving desired results. Health Affairs. 2012;31:843-851.
- Ehman KM, Deyo-Svendsen M, Merten Z, Kramlinger AM, Garrison GM. How preferences for continuity and access differ between multimorbidity and healthy patients in a team care setting. Journal of Primary Care and Community Health. 2017;1-5.
- Sinaiko AD, Rosenthal MB. The impact of tiered physician networks on patient choices. Health Services Research. 2014;49:1348-1363.
- Laurant M, Reeves D, Hermens R, Braspenning J, Grol R, Sibbald B. Substitution of doctors by nurses in primary care. Cochrane Database of Systematic Reviews 2005:CD001271.
- Liu H, Robbins M, Mehrotra A, Auerbach D, Robinson BE, Cromwell LF, Roblin DW. The impact of using mid-level providers in face-to-face primary care on health care utilization. Medical Care. 2017;55:12-18.
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: National Academy Press, 2001.
- U.S. Census Bureau. Current Population Survey, 2014 Annual Social and Economic Supplement. Available from: https://www2.census.gov/programs-surveys/cps/techdocs/cpsmar14R.pdf.