Michael Karamardian*, Perelman School of Medicine and The Wharton School, University of Pennsylvania; Ekta Jagtiani*, University of Pennsylvania; Ankit Chawla*, IESE Business School, and Ingrid M. Nembhard, The Wharton School, University of Pennsylvania
Contact: ingridn@wharton.upenn.edu
What is the message? Private equity (PE) ownership in healthcare is largely associated with lower performance on health system aims including patient health outcomes, process quality, and costs for patients and other payers, though notable positive impacts include better cost efficiency for care providers and possibly lower readmissions for patients. Given these results, greater managerial attention is needed to ensure that financial and operational efficiency is not obtained at the expense of other important responsibilities of health systems, which may be possible as some studies indicate that select PE firms perform well across aims, suggesting that management priorities and systems matter.
What is the evidence? We conducted a systematic review of quantitative empirical research on PE’s impact in healthcare published from January 2000-April 2024 in leading health services, business, and economics databases. Our review incorporates a secondary analysis of Borsa et al.’s 2023[1] systematic review (covering 32 articles through April 2023), our primary analysis of articles published subsequently (N=8 from April 2023 to April 2024), and studies forthcoming for presentation at the prestigious AcademyHealth Annual Research Meeting (N=7; June 2024).
Timeline: Submitted: May 14, 2024; accepted after review May 16, 2024.
Cite as: Michael Karamardian, Ekta Jagtiani, Ankit Chawla, Ingrid M. Nembhard. 2024. An Update on Impacts of Private Equity Ownership in Health Care: Extending A Systematic Review. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
* Denotes that authors contributed equally as lead authors of this article
Acknowledgements: We are grateful for the expert assistance of Marcella Barnhart, the Zilberman Family Director of the Lippincott Library of The Wharton School, who performed our databases searches and helped us process the results. Tina Horowitz provided expert administrative and research assistance that saved the day; we are beyond grateful for her and that. We also thank Stephen Sammut, MBA, DBA (Senior Fellow in the Health Care Management Department of The Wharton School and Chair of the Industry Advisory Board of Alta Semper Capital, a private equity impact fund focused on health care investing in Africa), who participated in early conversations about the private equity landscape to help orient us. Kevin Schulman, MD (Professor of Medicine, Clinical Excellence Research Center at the Stanford University School of Medicine and Professor of Operations, Information and Technology at the Stanford Graduate School of Business) provided inspiration and motivation for this work.
Since 2012, private equity (PE) firms have completed more than 8,000 transactions involving healthcare entities, with an estimated combined value of nearly $1 trillion.[2] Using money from investors, these firms have acquired healthcare services entities (e.g., hospitals, medical groups, nursing homes), whom they then typically charge a management fee and incur sizable debt against. They quickly turn around these organizations, selling them to make profit for their investors, normally within five to 10 years.[3] An estimated 788 PE transactions occurred in 2023 alone just within the healthcare services sector ─ our focal sector in this article ─ making 2023 the third highest year by deal count, even though the count declined relative to recent years. [4]
PE transactions within healthcare services ─ most recently documented in Ma et al.’s [5] article in this issue of HMPI ─ are part of what is labeled the “financialization of health.”[2] This label captures the growing influence of financial incentives, markets, motives, and institutions in the functioning of the healthcare industry.[2] This influence is growing internationally,[1,8] which has sparked the interest of organizational leaders, media, policymakers, clinicians, and researchers who all ponder whether PE investment in healthcare services is good or bad for the industry. [6, 7, 8]
In theory, on the positive side, PE firms may improve the cost and efficiency of healthcare delivery given the inherent financial incentives of their workflow. Because they aim to optimize investment returns, they frequently implement substantial restructuring of acquired entities to generate improvements in these areas.[3, 9] Conceivably, restructuring can also deliver patient care benefits if prioritized as well.[10] However, several reports indicate troubling trends associated with PE ownership including higher bills for patients, outsized growth in earnings for insurers, and high bankruptcy rates, especially in communities that serve a large proportion of low-income and uninsured patients, leading to greater difficulty in accessing care.[7, 11, 12] Over 20% of healthcare entities that filed for bankruptcy in 2023 were owned by PE firms,[13, 14] prompting concern that PE ownership may leave communities depleted of healthcare. This concern has intensified as PE-backed Steward Health Care, the largest physician-led hospital operator in the United States (U.S., with 30 hospitals), filed for bankruptcy in May 2024, unable to pay its $750 million debt.[15, 16] Steward, formerly renowned for its outstanding performance in the value-based Medicare Shared Savings Program (MSSP),[17] had served as a compelling example of the positive influence of PE. After PE acquisition, Steward transformed into one of the major for-profit U.S. hospital systems, expanding healthcare nationally. Then, under pressure to achieve financial profit, Steward underwent substantial operational restructuring, primarily emphasizing cost reduction and division optimization, but remained unable to repay its sizable PE-linked debt. See related article by Kumar in this issue of HMPI.
The recent events and growth of PE have prompted many commentaries, conferences, and case studies on PE’s impact in healthcare.[18, 19, 20, 21, 22, 23, 24, 25, 26] Recently, they also spurred a systematic review of all related empirical research published from 2000 to 2023. That review by Borsa et al.[a][1]aimed to provide an evidence-based summary of the impact of PE ownership with respect to health outcomes, costs to patients or payers, cost to operators, and quality. In sum, Borsa et al. found that PE ownership is “often associated with harmful impacts on costs to patients or payers and mixed to harmful impacts on quality” (p. 1). This largely negative conclusion has been affirmation for some within the healthcare community. Others wonder whether the conclusions would stand with additional data and finer-grained analysis of study outcome variables.
To answer these open questions, we conducted a systematic review with three aims: 1) to include data from the year since Borsa et al. (April 2023-April 2024) to assess if the patterns identified by them persist; 2) to assess the influence of PE on patient health outcomes and care quality as a single category, distinct from process quality enablers (a departure from Borsa et al. that we explain in Methods below); and 3) to investigate whether the effects of PE ownership differ by PE firm. Our analysis updates the existing systematic review of the evidence of PE’s impact and adds nuance through subset analyses of data. It thus is both a replication and expansion to contribute to a detailed and current evidence base on a key topic in healthcare management today, enabling knowledge to guide policy and practice.
Given our aims of providing a detailed and updated systematic review of empirical research on PE, our review consisted of three components. In the first component, we abided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement[27] and used our search procedures to bring Borsa et al.’s review forward in time. Specifically, with the assistance of our university librarian, we searched for English-language articles in PubMed (MEDLINE and MEDLINE In-Process), Scopus, and Web of Science for the full year following Borsa et al.’s, that is, from April 16, 2023 (the final date of their search) to April 15, 2024. In PubMed, a search was conducted for “private equity”. For Scopus and Web of Science, the search strategy included various bibliographic fields (title, abstract, and author keywords in Web of Science; and title, abstract, and keywords in Scopus) using the terms health* or hospital* or physician* or doctor* or medical or nursing or hospice or ambulatory or “long term care” and “private equity.”
To limit the possibility that we missed relevant research published by business or economics scholars, we added search of Business Source Complete, ABI/Inform and EconLit. As these sources were not included in the Borsa et al. article, we expanded the search of these to begin in 2000 to align with Borsa et al., agreeing that PE acquisitions before that time were likely to be less relevant to current events. Our search terms were the same as for Web of Science. Identified articles were reviewed by our librarian to assess whether they met our three inclusion criteria: (1) studied any form of PE ownership, (2) utilized empirical, quantitative data, and (3) assessed the impact of PE ownership in a healthcare delivery setting using statistical analyses. Our librarian uploaded articles that met criteria to a shared Box for our full review and data extraction. She also uploaded Excel files with the list of all articles from each database that documented reasons for exclusion/inclusion and provided a link to the article. Excluded articles focused on non-healthcare related effects, did not include statistical analyses, analyzed predictors of PE ownership, or were commentary/editorial or news pieces.
The second component of our review aimed to capture studies forthcoming in publications in an effort to be as current as possible. To identify these, we conducted an online search of the 2024 AcademyHealth Annual Research Meeting (ARM) program.[28] AcademyHealth is the premier professional association for health services researchers, policymakers, and healthcare practitioners and stakeholders in the U.S. Selection for presentation during its research meeting occurs through blind, committee review of abstracts, with selection for podium presentation limited to research assessed as most rigorous and impactful. We searched the 2024 program using “private equity” and applied the same eligibility criteria used in the first component of our search methods.
The third and final component of our review consisted of revisiting the 32 articles identified by Borsa et al. as evaluating the impacts of PE ownership on at least one category of health outcomes, costs to patients or payers, cost to operators, or quality, or a combination of these factors. We revisited these articles to ensure that our categorization of impacts for new research aligned with theirs in order to create continuity as the field of study and analysis grows.
Our data analysis and extraction had two phases. In the first phase, we focused on establishing the categories of impact that would be the focus of our review. We used Borsa et al.’s categories (health outcomes, costs to patients or payers, cost to operators, and quality) as our starting point and also allowed our “fresh eyes” to consider whether additional or more fine-grained categories would be valuable additions to present. With this objective, one team member (EJ) documented the results in detail from 20 articles in our dataset (the first 12 in Borsa et al. and the first 8 published since then) and noted themes across them, all in an Excel file. Next, two additional members of the team (MK and AC), both with clinical and business training, reviewed the Excel file independently and then jointly to create the list of categories of impact to be used for the analysis of all articles. All authors met to finalize the categories, which are presented in Table 1.
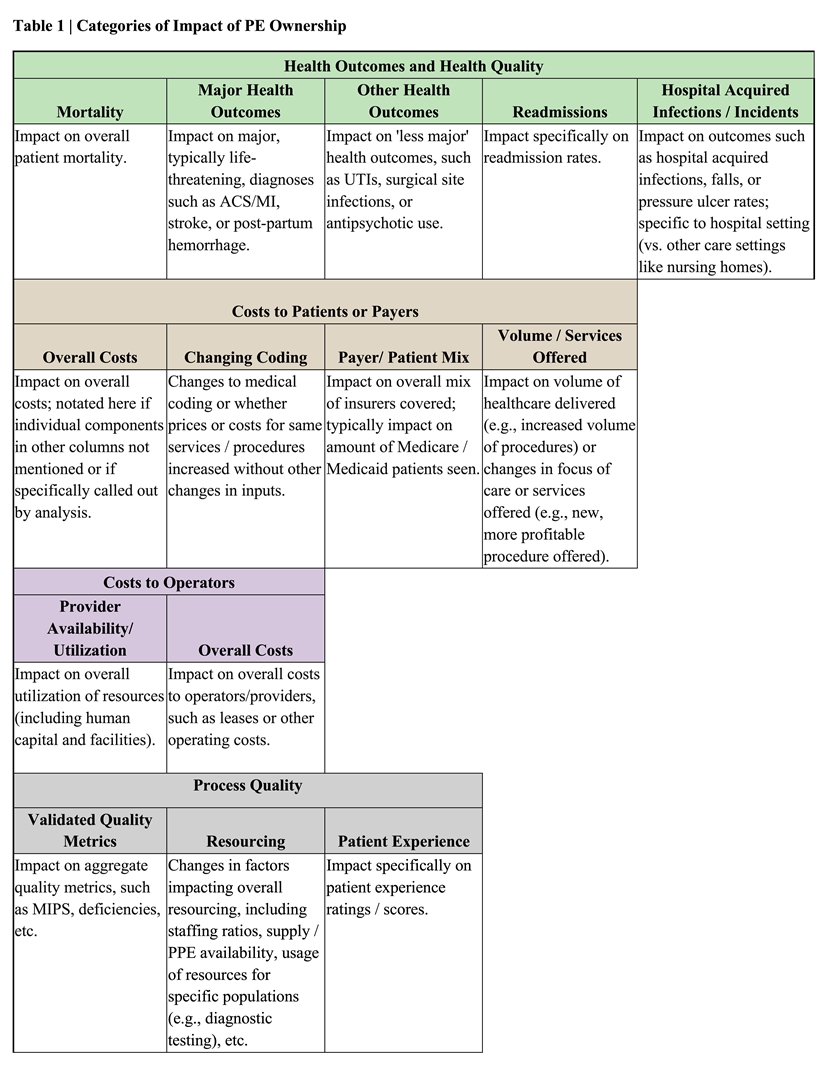
A notable distinction between our categories of impact and those contained in Borsa et al.’s is that we chose to differentiate within the category of Quality, drawing upon Donabedian’s[29, 30] taxonomy. Specifically, we distinguished between impacts related to patient health (often regarded as technical quality of care and labeled here as “Health Outcomes and Health Quality”) and impacts related to enablers of care delivery (often regarded as process and labeled here as “Process Quality”). We see value in distinguishing these impacts because, although process and outcomes measures are often loosely-coupled, systems that affect them and interventions to improve them can differ. Our differentiation led to reclassification of some measures from Quality in Borsa et al. (i.e., surgical site infections and (in)appropriate antipsychotic use) to Health Outcomes and Quality here. That resulted in more specificity as the broad category of Quality became more precisely Process Quality enablers. Within the Process Quality and Health Outcomes and Quality categories, we took the added step of documenting sub-categories to add another level of precision to our main results presentation. Similar content is captured in Borsa et al.’s supplement.
Once we finalized our categories of impact as noted in Table 1, we divided the articles/abstracts identified from our three (search) components among our three lead authors for data extraction. Each article/abstract was reviewed by at least two team members to ensure accuracy and consistency in categorization. Reviewers for each article extracted the following study information: author, year of publication, article title, research question/objective, country, healthcare setting, sample, study design, time period of analysis, sample size, named PE firm (if applicable), impact(s) assessed, significance of impact based on p-value < 0.05 as significant, and indicator for whether a category changed from Borsa et al. Information was recorded in Excel spreadsheets. The full authorship team then met on four occasions to review the data to identify patterns and answer the research questions.
Our three search strategies yielded 47 articles/abstracts for analysis, 15 of which were additions to the 32 articles previously identified by Borsa, for a research growth rate of 47 percent in just one year for studies meeting our inclusion criteria. Of the 15 new articles, eight were identified from among 57 new articles retrieved through our database search of articles since Borsa et al. and seven were identified through search of the AcademyHealth program, which contained 14 studies. These additions from AcademyHealth were largely by research teams (5 out of 7) with a track record of publishing empirical research on PE, adding credibility to our inclusion of their forthcoming work. Excluded articles obtained from both searches had failed to meet our inclusion criteria. Of note, no new articles were identified in our added databases; either nothing new had been published or articles were already included in Borsa et al., demonstrating the completeness of their 2023 search.
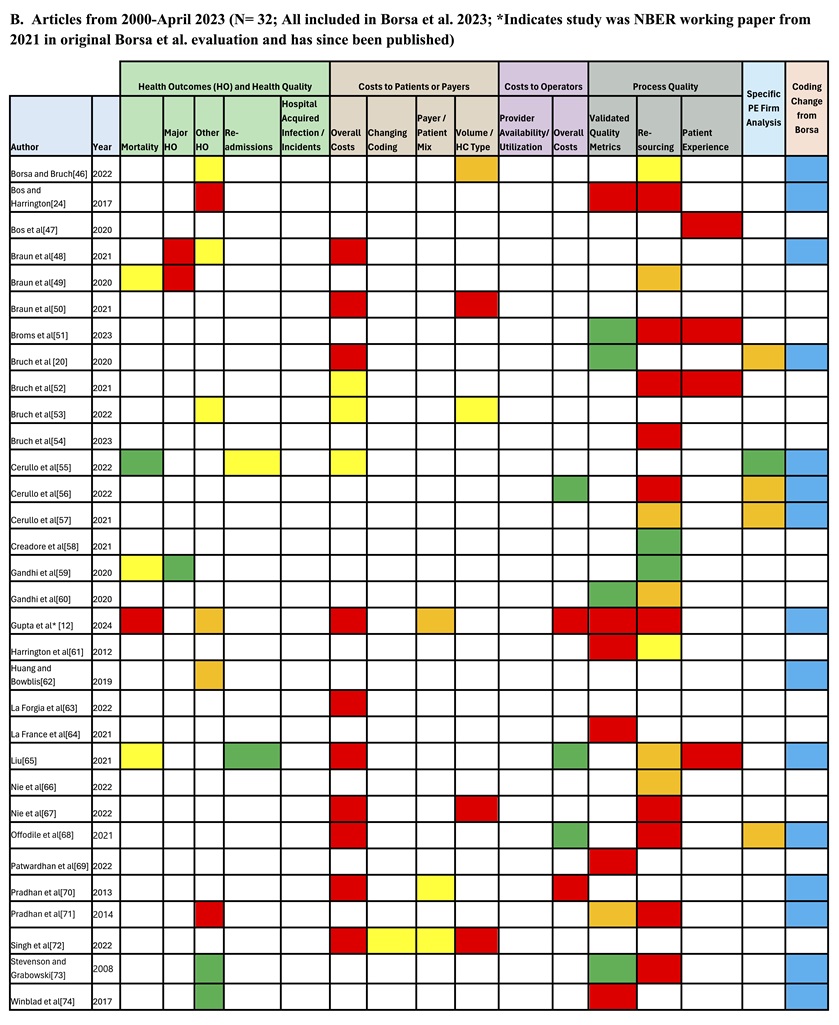
Table 2 shows the impacts reported across the 47 articles/abstracts published from 2000-April 15, 2024. Part A shows the results for the research published in the most recent year, whereas Part B shows the results for articles contained in Borsa et al. and whether a classification change had occurred based on categories in Table 1. These tables also indicate the five studies that assessed whether results varied by PE firm, comparing HCA-ownership relative to other owners.
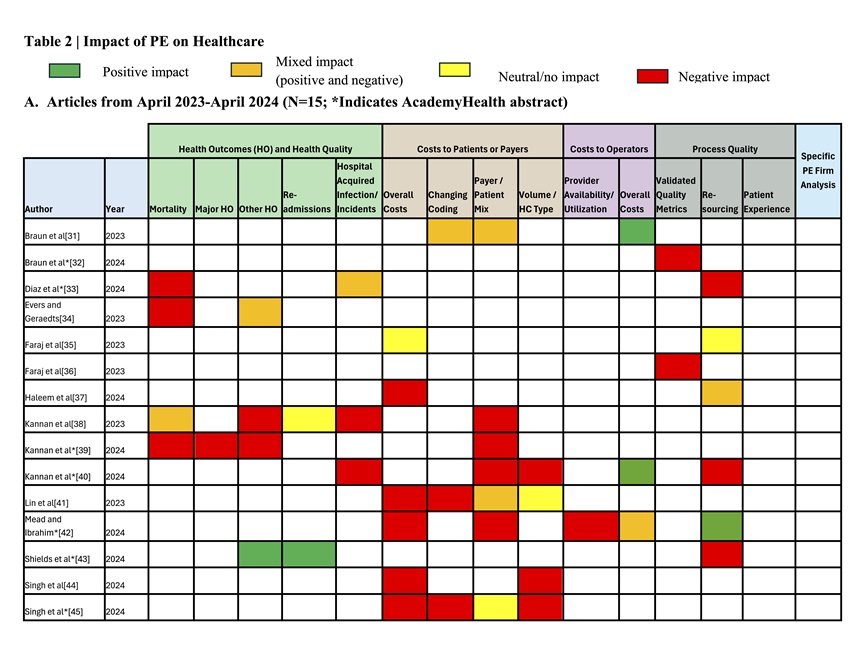
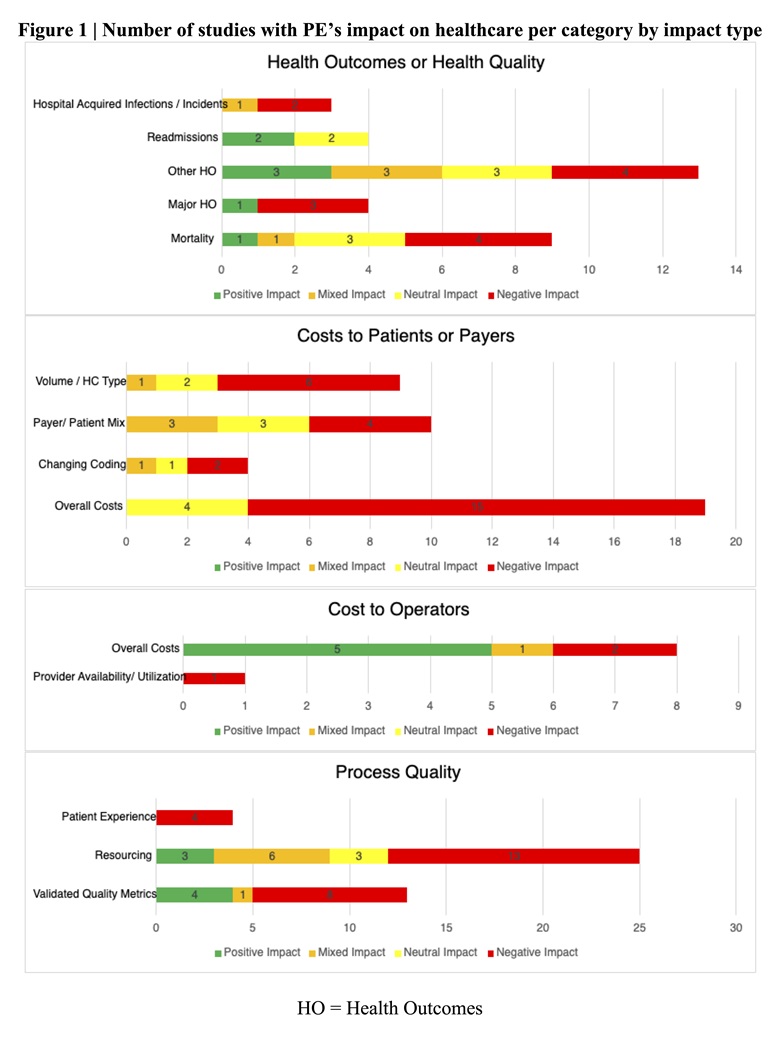
Within this category, the majority of effects assessed in studies during the last year indicate unfavorable health consequences for patients. Specifically, studies indicate that patients served by PE-owned entities have higher rates of mortality, major and other adverse health outcomes, and complications such as hospital acquired infections. The most recent year’s data reinforces the negative view of PE’s impact on health outcomes overall, as there were relatively few articles citing positive impact, and they often indicated negative impacts as well. Just one study in the past year indicated uniformly better health outcomes, with the patients in that study having lower readmission rates and better other health outcomes (e.g., improved rates of urinary tract infections).[43] Moreover, as Part B of Table 2 shows, we observe more studies reporting negative and neutral impacts compared to Borsa et al. in this category due to our decision to include health quality impacts in this category, which shifted some studies into this category. Thus, across the entire time frame for review, the data suggests that PE ownership is associated primarily with negative impacts on patient health outcomes and health quality, although there are studies indicating positive and/or neutral effects.[43, 57, 60, 73, 74] This is seen in both Table 2 and Figure 1, which presents the number of studies that report each type of impact (positive, mixed, neutral, or negative) within each category.
Studies to date overwhelmingly indicate that PE ownership is also associated with higher costs to patients and payers. Across time periods and all sub-categories assessed (overall costs, billing codes (e.g., changing to higher paying codes), payer/patient mix (e.g., shifting away from costly patients), and volume of more expensive services offered/provided), the preponderance of evidence indicates negative financial effects for these two groups, with a recurring pattern of higher expenses for payers and patients linked to service fee growth after a PE acquisition.[41, 63, 68] Studies also suggest that financial access to care is hindered as changes to payer/patient mix occur that typically involve reduced percentages of Medicare, Medicaid, or Dual-Eligible patients being covered, [38, 39, 42],, a pattern highlighted in the most recent year of studies, although evidence is mixed. To the extent studies indicated positive effect on costs for these two groups, they also included negative effects. Thus, overall, the most recent year of results is consistent with the results of Borsa et al., with the most recent studies expanding the field by offering mechanisms for the overall cost growth indicated by the 2000-2023 articles. Notably, increased costs were not often accompanied by better Health Outcomes or Health Quality; only one [65] of three studies that examined this possibility [12, 48, 65] indicated such betterment.
Studies in this category indicate a mix of positive and negative effects on cost for operators (i.e., operational expenses). That said, this is the only category with significant evidence of positive impact, relative to the number of studies. While several studies indicate cost reductions resulting from greater efficiencies,[31, 40, 55, 65, 68] there was counterevidence that in some cases PE ownership actually raised costs such as lease costs,[12] which may not be directly linked to improved service delivery or patient care. Additionally, one of the studies in the past year, the first to consider how provider availability or utilization is impacted, found a negative effect, i.e., lower utilization that increased cost for operators.[42]
Overall, process quality had largely mixed impact, though notably many studies reported significantly decreased staffing levels at PE-owned facilities.[12, 24, 40, 43, 51, 52, 55, 68, 71, 73] The sub-component within process quality where analysis shows that PE firms perform most positively is in their impact on Validated Quality Metrics.[20, 51, 59, 73 ] Notably, no studies reported any positive impacts on patient experience scores.
Five articles contained a sub-analysis to parse the effect that PE acquisition of HCA-associated hospitals had on various impact metrics. All of these articles were included in the Borsa et al. review but had not been examined separately to assess whether specific PE firm management moderated the impact of ownership. Notably, HCA’s impact on health outcomes, though only analyzed in one study, [55] was significant on the important metrics of 30-day patient mortality and mortality from myocardial infarction (heart attack). While impacts on costs and process quality were mixed,[20, 56, 57, 68] the significant and positive findings provide evidence of potential variance in impact due to specific PE firm ownership. We observed no systematic differences in impacts based on healthcare setting or specialty.
The primary purpose of our review was to provide the most up-to-date summary of research on PE’s impact on healthcare delivery settings. In multiple venues, we had heard or read debate about whether PE is good or bad for healthcare – for patients, the workforce, organizations, and ultimately the system. Borsa et al. had admirably conducted an extensive systematic review of the literature from 2000 to 2023. It left a negative impression of PE ownership and raised the question of whether newer, additional studies would provide results that offer a more mixed or favorable impression. Our review, which adds a year of studies to Borsa et al.’s and reports on more sub-categories of impacts as part of the main analyses, reinforces Borsa et al.’s findings. This is true whether just the 15 new studies are considered or the entire set of 47 studies.
Our review confirms negative associations across three of the four categories of impacts identified: health outcomes and health quality, cost to patients and payers, and process quality enablers. The negative associations appeared stronger in the category of health outcomes and health quality once we shifted adverse event quality measures to be alongside health outcomes. The one categorical exception to negative-dominant impacts occurs for cost to operators, which had the most evidence of positive effects. Gains in this area indicate that PE ownership is delivering on this expectation. A modus operandi of PE is to increase operational efficiency and reduce costs so the acquired is sellable at a profit for original investors.[2, 3, 7],
The results of this review add to concern about the growth of PE in healthcare. They imply that this form of financialization in healthcare can bring cost efficiency for the acquired operator but also significant detrimental effects for patients on multiple dimensions, some of which may result from declines in organizations’ process quality, as processes influence outcomes in many instances, meaning they too deserve attention.[29,30] Given the negative findings for process quality and outcomes, it is not surprising that no study showed improved patient experience scores after PE acquisition. Lack of improvement and negative effects may have several potential reasons, ranging from PE’s inherent focus on short-term profitability and thus cost-cutting actions to less tangible causes like disruptions to organizational culture due to restructuring and operational ‘optimizations’, which can undermine service delivery.[
Our findings, however, are not wholly damming of PE. At least two sets of findings suggest that PE can have beneficial effects. The first are the subset analyses of HCA versus non-HCA PE-owned hospitals, which showed significantly better 30-day patient mortality rates and mortality from myocardial infarction (heart attack) for the HCA hospitals.[55] The second indicator is the many mixed results studies (orange boxes in Table 2) alongside the few positive impact studies (green boxes) such as for readmission rates.[43, 65] While the number of these studies is far fewer than the negative studies, as evident in Figure 1, their existence is noteworthy. They imply positive possibility and that more research is needed that examines under what conditions PE is helpful. The HCA studies, in particular, beg the question: What exactly do PE firms that perform well in areas beyond own-cost management do? We know that firms operate differently and management matters in healthcare.[75] It may be time to study how different PE firms in healthcare manage differently, the implications of those choices, and what shifts in operational and managerial strategy are possible to allow PE-owned entities to not only deliver efficiency but also other health system aims, assuming that investors are willing to accept this challenge. Study of over 15,000 firms across industries found that PE firms are better managed than government, family, and privately owned firms, and have similar management to publicly listed firms, in the developed and developing world. They tend to have strong people management (hiring, firing, pay, and promotions) and monitoring management practices (lean manufacturing, continuous improvement, and monitoring).[76] Therefore, it may be that there is lurking potential in PE firms for healthcare. Current negative impacts may be the result of the PE model itself or insufficient experience with or adaptation of this innovation to the current era of healthcare. Innovation and organizational learning research both indicate that negative results are common early in the use of new innovations; time is often needed to learn appropriate strategies for the setting.[77, 78] Though PE investment in healthcare services has been occurring for decades and the recent volume of transactions appears motivated by the same uncertainty, goals, and motivations of past private investment in healthcare,[7] the current era differs in ways (e.g., more burned out workforce, players, technology-enabled activities, and reserves for capitated business amid expectations for transparency and value-based care) that may present novel contexts for PE operators. Thus, additional study of specific PE-firm behavior is needed to get us closer to understanding the variation in impacts observed across studies.
Our study’s (re)classification of specific measures into separate categories of quality, specifically ‘process’ and ‘health outcomes’ quality, and examination of the sub-categories within them allows for nuanced understanding of effects. While completely reasonable to group all under “quality,” the two levels of categorization allowed us to observe the distinct association of PE ownership with patient health (for example, we felt patient mortality effects deserve to be highlighted) and observe the association across the spectrum from the most serious (e.g., mortality) to minor health effects. It also allowed us to appreciate the distinction of effects on process quality enablers (e.g., resources), which can affect patient health but also have separate effects (e.g., affecting staff retention rates) that may not impact patient health. The categories presented in Table 1 may be used to guide future studies and serve as a starter checklist for PE performance.
While we endeavored to capture all published research and forthcoming articles since Borsa et al., it is possible that studies were missed despite our broad search for “private equity,” search of databases across scholarly fields, and search within the program for the most prominent health services research conference. Another potential limitation of this work is that its conclusions are based on studies that vary in their rigor and bias. We did not document these threats for the new articles. Borsa et al. had already documented such variation for the studies included in their analysis. Although we observed that several of the new articles used more robust study designs (e.g., allowing for difference-in-differences analyses), across the dataset, the threats to our findings remain. Several studies did not account for confounders that may impact the results, such as pre-acquisition financial health, market conditions, and regulatory modifications. This hinders attribution of identified impacts to PE ownership. Additionally, the included studies exhibit substantial heterogeneity in scope, setting, and measurement. This has the advantage of allowing assessment of generalizable patterns but also means that setting-specific effects (positive or negative) are obscured, especially given the few studies in any context. Given the growth in studies in one year, however, we are optimistic that the research on PE will continue to grow such that robust conclusions about the impact of PE in healthcare generally and with nuance will be gained.
The increase in empirical study following Borsa et al.’s work suggests an ongoing need for comprehending the influence of PE on healthcare. Research to date shows that PE ownership can deliver the cost efficiency gains promised but also that positive impacts on patient health outcomes, process quality, and cost to patients and payers do not naturally accompany these gains. Rather, much of existing evidence indicates negative impacts in these areas. There is also some indication, however, that management can matter. The positive health impacts found for readmission rates and in HCA-hospital sub-analyses suggest the possibility for PE ownership to deliver on cost and quality aims for patients and organizations. This likely depends on organizational priorities and management systems implemented.
[1] Borsa A, Bejarano G, Ellen M, Bruch J D. Evaluating trends in private equity ownership and impacts on health outcomes, costs, and quality: systematic review BMJ 2023; 382:e075244 doi:10.1136/bmj-2023-075244
[2] Bruch JD, Roy V, Grogan CM. The financialization of health in the United States. New England Journal of Medicine. 2024 Jan 11;390(2):178-182. doi: 10.1056/NEJMms2308188. PMID: 38197821
[3] Cutler DM, Song Z. The new role of private investment in health care delivery. JAMA Health Forum. 2024;5(2):e240164. doi:10.1001/jamahealthforum.2024.0164
[4] Olsen, E. Healthcare PE deals third-highest on record in 2023: Pitchbook. Healthcare Dive. Feb. 12, 2024. https://www.healthcaredive.com/news/healthcare-private-equity-deals-2023-pitchbook/707245/?utm_medium=email&utm_source=rasa_io&utm_campaign=newsletter
[5] Ma LW, Buckmann C, Shah SA, Schulman KA. Healthcare Private Equity: A Review of Key Case Studies and Recommendations for Effective, Equitable Private Investment in Healthcare. Health Management, Policy and Innovation (www.HMPI.org). 2024. Volume 9, Issue 2.
[6] Scheffler RM, Alexander L, Fulton BD, Arnold DR, Abdelhadi OA. Monetizing medicine: private equity and competition in physician practice markets. American Antitrust Institute. 2023 Jul 10.
[7] Pauly MV, Burns LR; Equity Investment in Physician Practices: What’s All This Brouhaha?. Journal of Health Politics Policy Law 2024; 11186103. doi: https://doi.org/10.1215/03616878-11186103
[8] Andersen JL. Impact Of Private Capital And Financialization On Health Equity: A Response To Enekwechi. Health Affairs Forefront. 2024.
[9] Appelbaum E, Batt R. Private Equity Buyouts in Healthcare: Who Wins, Who Loses? Institute for New Economic Thinking Working Paper Series. Published online 2020:1-115. https://doi.org/10.36687/INETWP118
[10] Enekwechi A. Private Capital Is A Key Component To Improving Health Equity. Health Affairs Forefront. 2023.
[11] Hamby, C. Health Insurers’ Lucrative, Little-Known Alliance: 5 Takeaways. The New York Times (April 7, 2024).
[12] Gupta A, Howell ST, Yannelis C, Gupta A. Does private equity investment in healthcare benefit patients? Evidence from nursing homes. National Bureau of Economic Research, 2021. doi:10.3386/w28474.
[13] Private Equity Stakeholder Report. (2024). Private Equity Healthcare Bankruptcies are on the Rise. Accessed May 7, 2024: https://pestakeholder.org/private-equity-healthcare-bankruptcies-are-on-the-rise/
[14] Bankruptcies Jump At Private Equity-Owned Healthcare Companies. (n.d.). Accessed May 1, 2024. https://www.medcentral.com/biz-policy/bankruptcies-jump-among-private-equity-owned-healthcare-companies
[15] Steward health care finalizing financing deal with medical properties trust to support its restructuring. Press Release May 6, 2024. https://www.steward.org/newsroom/2024-05-06/steward-health-care-finalizing-financing-deal-medical
[16] Vogel, S. Steward Health Care files for Chapter 11 bankruptcy. Healthcare Dive (May 6, 2024) https://www.healthcaredive.com/news/steward-health-care-files-chapter-11-bankruptcy/714050/?utm_medium=email&utm_source=rasa_io&utm_campaign=newsletter
[17] Medicare shared savings program. Steward.org. Accessed May 7, 2024. https://www.steward.org/domain-specific/720191/MedicareACO/MSSP
[18] Patouillard E, Goodman CA, Hanson KG, Mills AJ. Can working with the private for-profit sector improve utilization of quality health services by the poor? A systematic review of the literature. International Journal for Equity and Health. 2007;6(1). doi:10.1186/1475-9276-6-17
[19] Beyer KM, Demyan L, Weiss MJ. Private equity and its increasing role in US healthcare. Advances in Surgery. 2022;56(1):79-87. doi:10.1016/j.yasu.2022.02.003
[20] Bruch JD, Gondi S, Song Z. Changes in hospital income, use, and quality associated with private equity acquisition. JAMA Internal Medicine. 2020;180(11):1428-1435. doi:10.1001/jamainternmed.2020.3552
[21] Ivashina V, Lerner J. Pay now or pay later?: The economics within the private equity partnership. Journal of Financial Economics. Published online 2016. doi:10.2139/ssrn.2757039
[22] Scheffler RM. Soaring Private Equiry Investment in the Healthcare Sector: Consolidation Accelerated, Competition Undermined, and Patients at Risk.; 2021.
[23] Powers BW, Shrank WH, Navathe AS. Private equity and health care delivery: Value-based payment as a guardrail? JAMA. 2021;326(10):907. doi:10.1001/jama.2021.13197
[24] Bos A, Harrington C. What happens to a nursing home chain when private equity takes over? A longitudinal case study. Inquiry. 2017;54:004695801774276. doi:10.1177/0046958017742761
[25] Gondi S, Song Z. Potential implications of private equity investments in health care delivery. JAMA. 2019;321(11):1047. doi:10.1001/jama.2019.1077
[26] Hunter BM, Murray SF. Deconstructing the financialization of healthcare. Development and Change. 2019;50(5):1263-1287. doi:10.1111/dech.12517
[27] Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
[28] AcademyHealth Annual Research Meeting (ARM) program 2024. Baltimore, MD; June 2024.
[29] Donabedian A. The quality of care. How can it be assessed? JAMA. 1988 Sep 23-30;260(12):1743-8.
[30] Donabedian A. Evaluating the quality of medical care. Milbank Quarterly. 2005;83(4):691-729.
[31]Braun RT, Unruh MA, Stevenson DG, et al. Changes in diagnoses and site of care for patients receiving hospice care from agencies acquired by private equity firms and publicly traded companies. JAMA Network Open. 2023;6(9):e2334582. doi:10.1001/jamanetworkopen.2023.34582
[32] Braun RT, Soltoff, A, Unruh, M, Stevenson, D, Casalino, L. Associations between Private Equity Firms’ and Publicly Traded Companies’ Ownership of Hospice and Caregiver Assessments of Hospice Quality. Unpubished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024).
[33] Diaz, A, Rohde, S, Kunnath, N, Dimick, J, Ibrahim, A. Association of private equity acquisition with inpatient general surgery outcomes. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024).
[34] Evers J, Geraedts M. COVID-19 risks in private equity nursing homes in Hesse, Germany – a retrospective cohort study. BMC Geriatrics. 2023;23(1):648. doi:10.1186/s12877-023-04361-8
[35] Faraj KS, Kaufman SR, Herrel LA, et al. The immediate effects of private equity acquisition of urology practices on the management of newly diagnosed prostate cancer. Cancer Medicine. 2023;12(24):22325-22332. doi:10.1002/cam4.6788
[36] Faraj KS, Kaufman SR, Herrel LA, et al. Acquisition of urology practices by private equity firms and performance in the Merit-based Incentive Payment System. Urology Practice. 2023;10(6):597-603. doi:10.1097/UPJ.0000000000000441
[37] Haleem A, Garcia A, Khan S, Shakelly P, Lee DJ. Access to sudden sensorineural hearing loss care at private equity‐owned otolaryngology clinics. Otolaryngology–Head and Neck Surgery. Published online 2024. doi:10.1002/ohn.665
[38] Kannan S, Bruch JD, Song Z. Changes in hospital adverse events and patient outcomes associated with private equity acquisition. JAMA. 2023;330(24):2365-2375. doi:10.1001/jama.2023.23147
[39] Kannan S, Stevens, J, Bruch, J, Song, Z. Hospital staffing, bed use, and patient outcomes after private equity acquisition. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024). AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024
[40] Kannan, S., Stevens, J, Song, Z. Hospital Staffing and Related Outcomes after Private Equity Acquisition. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024)
[41] Lin H, Munnich EL, Richards MR, Whaley CM, Zhao X. Private equity and healthcare firm behavior: Evidence from ambulatory surgery centers. Journal of Health Economics. 2023;91:102801. doi:10.1016/j.jhealeco.2023.102801
[42] Mead, M, Ibrahim, A. Private equity acquisitions of hospitals and changes in utilization and financial performance. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024).
[43] Shields, M, Yang, Y, Busch, S. Psychiatric hospitals are not immune to financialization: Private equity trends and its association with staffing and quality performance. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024).
[44] Singh Y, Aderman CM, Song Z, Polsky D, Zhu JM. Increases in Medicare spending and use after private equity acquisition of retina practices. Ophthalmology. Published online 2023. doi:10.1016/j.ophtha.2023.07.031
[45] Singh, Y, Song, Z , Polsky, D, Zhu, J. Increases in physician professional fees in private equity owned vs health system-affiliated gastroenterology practices. Unpublished paper. AcademyHealth Annual Research Meeting (Baltimore, MD, June 2024).
[46] Borsa A, Bruch JD. Prevalence and performance of private equity-affiliated fertility practices in the United States. Fertility and Sterility. 2022;117:124-30. doi:10.1016/j.fertnstert.2021.08.035
[47] Bos A, Kruse FM, Jeurissen PPT. For-profit nursing homes in the Netherlands: What factors explain their rise? International Journal of Health Services. 2020;50:431-43. doi:10.1177/0020731420915658
[48] Braun RT, Jung HY, Casalino LP, Myslinski Z, Unruh MA. Association of private equity investment in US nursing homes with the quality and cost of care for long-stay residents. JAMA Health Forum. 2021;2(11):e213817. doi:10.1001/jamahealthforum.2021.3817
[49] Braun RT, Yun H, Casalino LP, et al. Comparative performance of private equity-owned US nursing homes during the COVID-19 pandemic. JAMA Network Open. 2020;3:e2026702. doi:10.1001/jamanetworkopen.2020.26702
[50]Braun, RT, Bond AM, Qian Y, Zhang M, Casalino LP. Private equity in dermatology: Effect on price, utilization, and spending: Study examines the prevalence of private equity acquisitions and their impact on dermatology prices, spending, use, and volume of patients. Health Affairs (Millwood). 2021;40(5):727-735. doi:10.1377/hlthaff.2020.02062
[51] Broms R, Dahlström C, Nistotskaya M. Provider ownership and indicators of service quality: Evidence from Swedish residential care homes. Journal of Public Administration Research and Theory 2023:muad002.
[52] Bruch J, Zeltzer D, Song Z. Characteristics of private equity–owned hospitals in 2018. Annals of Internal Medicine. 2021;174(2):277-279. doi:10.7326/m20-1361
[53] Bruch JD, Nair-Desai S, Orav EJ, Tsai TC. Private equity acquisitions of ambulatory surgical centers were not associated with quality, cost, or volume changes. Health Affairs (Millwood). 2022;41(9):1291-1298. doi:10.1377/hlthaff.2021.01904
[54] Bruch JD, Foot C, Singh Y, Song Z, Polsky D, Zhu JM. Workforce Composition In Private Equity-Acquired Versus Non-Private Equity- Acquired Physician Practices. Health Affairs (Millwood). 42:121-129. doi:10.1377/hlthaff.2022.00308
[55] Cerullo M, Yang K, Joynt Maddox KE, McDevitt RC, Roberts JW, Offodile AC 2nd. Association between hospital private equity acquisition and outcomes of acute medical conditions among Medicare beneficiaries. JAMA Network Open. 2022;5(4):e229581. doi:10.1001/jamanetworkopen.2022.9581
[56] Cerullo M, Lin YL, Rauh-Hain JA, Ho V, Offodile AC 2nd. Financial impacts and operational implications of private equity acquisition of US hospitals: Study examines the impacts and operational implications of private equity acquisitions of US hospitals. Health Affairs (Millwood). 2022;41(4):523-530. doi:10.1377/hlthaff.2021.01284
[57] Cerullo M, Yang KK, Roberts J, McDevitt RC, Offodile AC 2nd. Private equity acquisition and responsiveness to service-line profitability at short-term acute care hospitals: Study examines private equity acquisition at short-term acute care hospitals. Health Affairs (Millwood). 2021;40(11):1697-1705. doi:10.1377/hlthaff.2021.00541
[58] Creadore A, Desai S, Li SJ, et al. Insurance acceptance, appointment wait time, and dermatologist access across practice types in the US. JAMA Dermatology. 2021;157(2):181-188. doi:10.1001/jamadermatol.2020.5173
[59] Gandhi A, Song Y, Upadrashta P. Have private equity owned nursing homes fared worse under COVID-19? SSRN Electronic Journal. Published online 2020. doi:10.2139/ssrn.3682892
[60] Gandhi A, Song Y, Upadrashta P. Private equity, consumers, and competition: Evidence from the nursing home industry. SSRN Electron Journal. Published online 2020. doi:10.2139/ssrn.3626558
[61] Harrington C, Olney B, Carrillo H, Kang T. Nurse staffing and deficiencies in the largest for-profit nursing home chains and chains owned by private equity companies. Health Services Research. 2012;47(1 Pt 1):106-128. doi:10.1111/j.1475-6773.2011.01311.x
[62] Huang SS, Bowblis JR. Private equity ownership and nursing home quality: an instrumental variables approach. International Journal of Health Economics Management. 2019;19(3-4):273-299. doi:10.1007/s10754-018-9254-z
[63] La Forgia A, Bond A, Braun AM. Association of Physician Management Companies and Private Equity Investment With Commercial Health Care Prices Paid to Anesthesia Practitioners. JAMA Internal Medicine. 2022;182:396-404.
[64] LaFrance A, Batt A, Appelbaum R. Hospital Ownership and Financial Stability: A Matched Case Comparison of a Nonprofit Health System and a Private Equity-Owned Health System. Advances in Health Care Management. 2021;20. doi:10.1108/S1474-823120210000020007
[65] Liu T. Bargaining with private equity: implications for hospital prices and patient welfare. SSRN. 38964. doi:10. 202110.2139/ssrn.3896410.
[66] Nie J, Hsiang W, Marks V, et al. Access to urological care for Medicaid-insured patients at urology practices acquired by private equity firms. Urology. 2022;164:112-117. doi:10.1016/j.urology.2022.01.055Nie J, Hsiang W, Lokeshwar SD, et al. 5
[67] Nie J, Hsiang W, Lokeshwar SD, et al. Association between private equity acquisition of urology practices and physician Medicare payments. Urology. 2022;167:121-127. doi:10.1016/j.urology.2022.03.045
[68] Offodile AC 2nd, Cerullo M, Bindal M, Rauh-Hain JA, Ho V. Private equity investments in health care: An overview of hospital and health system leveraged buyouts, 2003-17. Health Affairs (Millwood). 2021;40(5):719-726. doi:10.1377/hlthaff.2020.01535
[69] Patwardhan S, Sutton M, Morciano M. Effects of chain ownership and private equity financing on quality in the English care home sector: retrospective observational study. Age and Ageing. 2022;51(12). doi:10.1093/ageing/afac222
[70] Pradhan R, Weech-Maldonado R, Harman JS, Laberge A, Hyer K. Private equity ownership and nursing home financial performance. Health Care Management Review. 2013;38(3):224-233. doi:10.1097/HMR.0b013e31825729ab
[71] Pradhan R, Weech-Maldonado R, Harman JS, Hyer K. Private equity ownership of nursing homes: implications for quality. Journal of Health Care Finance. 2014;42.
[72] Singh Y, Song Z, Polsky D, Bruch JD, Zhu JM. Association of private equity acquisition of physician practices with changes in health care spending and utilization. JAMA Health Forum. 2022;3(9):e222886. doi:10.1001/jamahealthforum.2022.288
[73] Stevenson DG, Grabowski DC. Private equity investment and nursing home care: is it a big deal? Health Affairs(Millwood) 2008;27:1399-408.doi:10.1377/hlthaff.27.5.1399
[74] Winblad U, Blomqvist P, Karlsson A. Do public nursing home care providers deliver higher quality than private providers? Evidence from Sweden. BMC Health Services Research. 2017;17(1). doi:10.1186/s12913-017-2403-0
[75] Bloom, N., Sadun, R. and Van Reenen, J., Does management matter in healthcare. 2014. Boston, MA: Center for Economic Performance and Harvard Business School.
[76] Bloom N, Sadun R, Van Reenen J. Do private equity owned firms have better management practices?. American Economic Review. 2015;105(5):442-6.
[77] Keating E, Oliva R, Repenning N, Rockart S, Sterman J. Overcoming the improvement paradox. European Management Journal. 1999;17(2):120-34.
[78] Nembhard IM, Tucker AL. Deliberate learning to improve performance in dynamic service settings: Evidence from hospital intensive care units. Organization Science. 2011;22(4):907-22.
Notes
[a] As this work builds on Borsa et al.,[1] that work is mentioned often. To reduce citation fatigue due to repetition, we do not provide the citation for Borsa et al. at each mention after this one. All instances of Borsa et al., refer to Borsa A, Bejarano G, Ellen M, Bruch J D. Evaluating trends in private equity ownership and impacts on health outcomes, costs, and quality: systematic review BMJ 2023; 382:e075244 doi:10.1136/bmj-2023-075244
Lucy W Ma, Cyrus Buckman, Shreya A Shah, Stanford University School of Medicine and Graduate School of Business; and Kevin A Schulman, Stanford University School of Medicine and Graduate School of Business, and Clinical Excellence Research Center, Stanford University School of Medicine
Contact: lucywma@stanford.edu
What is the message? This paper introduces what private equity (PE) is, why healthcare became an attractive industry for investment, and how trends in PE healthcare investments have shifted over time in response to various regulating factors, illustrated through three noteworthy PE cases. We hypothesize that the initial interest of PE in certain healthcare services derived from intrinsic qualities of the healthcare sector, macroeconomic and political factors. In addition, we speculate that the trends in PE shifting away from traditionally popular deal types, and sub-industries such as emergency medicine, anesthesiology, and air ambulances, are due to regulatory changes, including the No Surprises Act (NSA) and legal action by governing bodies, as well as macroeconomic effects from the COVID-19 pandemic and interest rate fluctuations. Finally, we emphasize the importance of aligning incentives in PE and healthcare to synergize their mutual impact, generating greater profitability and sustainably high-quality care delivery for patients to minimize costs and improve outcomes. We recommend a combination of public policy and research on the long-term impacts of PE’s new strategic investments to hold the industry accountable and inform continued regulation.
What is the evidence? Our study uses press releases, news articles and investigative reports, and academic literature to illustrate the evolution of key PE strategies in healthcare. We draw takeaways about the unique and shared financial motives, associated investment risks, and critical populations who most often bear the consequences of both PE acquisitions and failures. The case studies we cover are KKR and Envision Healthcare (buyout), Welsh, Carson, Anderson & Stowe and U.S. Anesthesia Partners (add-on), and VBC-related deals (add-on, with unique shift in exit strategy), to illustrate landmark administrative responses to PE’s historic manipulation of healthcare acquisitions for profitability. Despite the skepticism around healthcare PE given historic investment scandals, we highlight several key regulatory and political recommendations that we believe, if executed proactively, could create a more sustainable future for private capital investment in healthcare.
Timeline: Submitted: May 17, 2024; accepted after review May 23, 2024.
Cite as: Lucy W Ma, Cyrus Buckman, Shreya A Shah, Kevin A Schulman. 2024. Healthcare Private Equity: A Qualitative Review of Investments in Healthcare Services and the Impact of the No Surprises Act of 2020. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
The healthcare sector has always been a critical area for private equity (PE) investments, given its significant impact on the economy and its potential for innovation and growth. For the past decade, PE firms have invested more than $1 trillion into U.S. healthcare.1 The appeal of healthcare for PE investors is multifaceted, driven by both industry-specific and macro trends. Within healthcare, the industry’s resilient “recession-proof” growth, high fixed demand, profitable loan restructuring, and the constant evolution and increasing commercialization of healthcare needs all present significant opportunities for value creation and sustainable growth. Additional macroeconomic aspects, especially in recent years, include low cost of capital from the Federal Reserve, a robust stock market, passage of the Affordable Care Act in 2010 which drove healthcare reform, Trump’s business-friendly administration boosting merger and acquisition (M&A) activity, and the COVID-19 pandemic’s acceleration of technology and healthcare delivery expansion.2
Rising in popularity during the 1980s, healthcare PE firms utilized leveraged buyouts (LBOs) most commonly to facilitate significant M&A activity among hospitals. This M&A wave, that continued into the 1990s and 2000s, arose from federal legislation that motivated hospital consolidation by incentivizing provider adoption of health information technology in order to facilitate more consistent, scalable care delivery.3 After Medicare introduced DRG-based payment systems in the 1980s, many hospitals also braced themselves for tightening operating margins and leaned into M&A in hopes of reducing costs and increasing revenue through economies of scale, streamlined operational efficiency, and increased market power. After initial LBOs to acquire hospitals, PE firms utilized a “buy and build” strategy to expand their platforms, and by February 2011, PE firms owned ten of the 15 largest for-profit hospital chains.
Nevertheless, healthcare PE activity has not always remained consistent. From macroeconomic trends such as changing interest rates and the COVID-19 pandemic that halted global operations, to regulatory shifts such as antitrust laws and the No Surprises Act (NSA), the PE industry has constantly needed to adapt their investment strategy in order to maintain their profitability in an evolving healthcare landscape. To fully understand how healthcare PE has responded to various changing influences and how sustainably the healthcare system can continue receiving private capital, we analyze three case studies that reflect critical changes in the industry’s primary investment themes over the past decade. Based on the responses of other players to these PE deals, we believe these case studies represent key inflection points in PE regulation and grant us valuable insight into the field’s relationship with governing regulatory, market, and financial forces.
Between 2010 to 2017, private equity deals were valued at $42.6 billion, reflecting a 187% increase within that period.4 A year later in 2018, the value of PE investments in healthcare had reached $100 billion, more than double the amount in 2017.5 Starting in the late 1990s to early 2000s, increased investment of PE in healthcare services likely derives from a few reasons: high growth potential and economic resilience (and thus high returns on investment [ROI] for PE firms), deregulation or regulatory changes, and the growing need for capital investment and management expertise in healthcare facilities and services.
Healthcare has always demonstrated significant resilience to economic downturn, even showing growth during some recessions. One reason is the stable demand given health insurance as a non-cyclical means of financial support for these services. Even during the 2008 financial crisis or the COVID-19 pandemic, healthcare needs did not stop, but in fact spiked significantly to the point of overwhelming the system during the pandemic, a time when most other significant industries nearly shut down.6 Another reason is the favorable demographic trend resulting from our aging population, especially the Baby Boomers (born between 1946-1964). As patients age, healthcare needs and demand for healthcare services both increase, supporting long-term growth in the healthcare sector by providing a steady demand for services ranging from preventative care to chronic disease management and geriatric care.7 Thirdly, the healthcare industry has always had significant regulatory and government support through funding mechanisms like Medicare and Medicaid and other subsidies, such as the tax treatment of employer health benefits.
Another factor that contributed to PE’s growing interest in healthcare investment was a series of regulatory shifts to accommodate new business and care delivery models. For example, the Stark Law prohibited physicians from giving referrals that could lead to financial gain for the physician or their immediate family, and the Anti-Kickback Statute prohibited the exchange of trading valuable items for referrals of patients participating in state or federal health programs. However, as our healthcare system has increasingly recognized the need for providers to work together to improve patient outcomes and efficiency, exceptions and waivers have been added to both laws to accommodate new healthcare delivery models, such as accountable care organizations (ACOs) and value-based care (VBC). This loosening of regulations has also opened up new investment opportunities for PE firms.
Certificate-of-Need laws, requiring government approval before opening or expanding healthcare facilities, have been relaxed or repealed in many states in order to promote competition, address service shortages, and reduce unnecessary regulatory burden. As a result, there has been room for increases in and expansions of healthcare facilities, often funded by PE firms as they rolled-up practices and aimed to improve operational efficiency.
Another trend, especially seen with the rise in telehealth services during the pandemic, is efforts to make it easier for providers to operate across state lines, expanding the market for many healthcare services. These developments, along with the typical lag time that policy often experiences in keeping up with these rapid developments, has increased the attractiveness of healthcare for PE investments.
Finally, PE firms provide significant capital investment to healthcare organizations that may not have access to other major forms of financing. This infusion of funds can greatly contribute to expanding facilities, upgrading technology and streamlining operational efficiency, and improving patient care services. In addition, group practices and hospital systems can encounter difficulty with management expertise and maintaining sustainable cash flows while providing the many services that patients need. Thus, on top of the capital they can provide, PE firms’ operational expertise is viewed as a significant benefit for small clinics that have difficulty scaling or healthcare systems struggling to stay afloat, even helping them become more competitive in concentrated areas, which can improve both patients’ continuity of care and job security of healthcare providers and staff.
The most common financing model used by PE in healthcare has traditionally been a leveraged buyout (LBO). The approach involves a financial transaction where a PE firm buys a majority stake in a healthcare company using a significant amount of borrowed money. PE firms look for healthcare companies with stable cash flows, potential for operational improvements, and a strong market position. These companies can range from hospitals and clinics to manufacturers of medical devices and pharmaceuticals. Upon identification of the target healthcare company, the PE firm finances the purchase through debt and the use of private equity funds, with debt being a significant portion of the financing deal (sometimes as high as 70%).5 The assets of the healthcare company being acquired—and sometimes the acquiring company’s assets—can be used as collateral for the loans.
After the acquisition, the PE firm works closely with the management of the healthcare company to improve operations, cut costs, and increase efficiencies with the goal of improving profitability (also referred to as “strategic dismantling”).3 The ultimate goal of an LBO is to sell the acquired company at a higher value than its purchase price. This can be achieved through various means, such as a sale to another company, a public offering, or selling it to another PE firm. LBOs in healthcare have been particularly attractive and feasible due to the sector’s generally stable and predictable cash flows, which are critical for servicing the debt incurred during the buyout.
Another investment model increasingly used by PE is the “platform and add-on,” or consolidation, approach. The goal is to build value by acquiring smaller companies around a larger, core company, known as the platform.8 The platform company serves as the foundation for the consolidation strategy, providing the infrastructure and management expertise necessary to integrate add-on acquisitions of smaller companies effectively. This “buy-and-build” method aims to create significant value through synergies, market expansion, diversified product offerings, and improved operational efficiencies and economies of scale.4,9
In 2018, Kohlberg Kravis Roberts (KKR), a globally leading PE firm, acquired Envision Healthcare Corporation, a provider of various healthcare services, post-acute care, and ambulatory surgery services, in an all-cash leveraged buyout (LBO) for $9.9 billion.10–12 Of that valuation, KKR financed $5.3 billion—more than 50%—with debt.13
Envision provided emergency department and inpatient, anesthesiology, and radiology services to over 300 healthcare facilities in 45 states and the District of Columbia, staffing other hospitals with their physicians. It was the biggest player in the physician outsourcing space, capturing 6% of the $41 billion emergency department and hospital-based physician market and 7% of the $20 billion anesthesiologist market.15
In order to service the debt and yield the returns promised to its investors, KKR deployed surprise medical billing.14 Health insurers establish contracts with providers (physicians and hospitals) that set up payment models for services. These contracts prohibit the provider from billing the patient for unallowed charges, essentially the amount of the provider charge that is above the negotiated payment rate, or the disallowed amount of the bill. Pursuing payment for these disallowed charges is a practice called balance billing. Out-of-network providers do not have a contract with a health plan, so they face no restrictions on balance billing for services. Providers are free to set their charges as they see fit without any further justification. In many states, courts uphold provider charges as the financial responsibility of the patient—even when these charges are grossly exaggerated or well above market prices.16
Many of Envision’s employed emergency room and radiology doctors had deliberately remained out-of-network providers for most health plans. Prior to the passage of the NSA in 2020, the company could surprise even insured patients with drastic medical costs and burden them with significant debt.5 These numbers ranged from $600, the average balance bill charge for an emergency room visit, to $100,000 for out-of-network providers that patients neither select for themselves nor have a choice to avoid.17
In 2019, Envision’s, and in turn KKR’s, reliance on surprise medical billing became clear through a series of media investigations and increasing scrutiny by health economists and advocacy groups, in particular focusing on its emergency room operations managed by its subsidiary, EmCare. A team of Yale health economists found that, after EmCare took over hospital emergency departments, patient care charges nearly doubled compared to those by previous physician groups, sending out-of-network bills at a rate of 62% compared with a national average of 26%.14 This represented a more than 81 percentage point increase in out-of-network billing rates at these hospitals that previously had low rates.15 In addition, average physician payments increased by 117%.15
Combined with widespread outrage from patients receiving surprise medical bills, Congress launched an inquiry into Envision after the National Bureau of Economic Research circulated the Yale study.15 Out of this investigation birthed the bipartisan bill that would ultimately become the NSA passed in December 2020. This legislation banned the practice of surprise medical billing and effectively destroyed Envision’s business strategy. The onset of the COVID-19 pandemic further strained Envision’s finances as the numbers of elective surgeries and ER visits—the main sources of out-of-network billing and revenue—plummeted. By April 2020, only one month after the pandemic’s onset, Envision began considering the need for debt restructuring and the increasing possibility of bankruptcy.18 In May 2023, Envision filed for Chapter 11 bankruptcy. KKR lost more than $5 billion.18,19
In 2023, the Federal Trade Commission (FTC) sued Welsh, Carson, Anderson & Stowe (WCAS), a private equity firm, for creating U.S. Anesthesia Partners (USAP) in 2012 to “roll-up” anesthesia practices in Texas and create a monopoly over the market and gain ultimate pricing power.20 The FTC claimed in its lawsuit that the PE firm’s actions violated key antitrust legislation, including the Sherman Act (which prescribes the rule of free competition), Clayton Act (which aims to prevent anti-competitive practices), and FTC Act (which outlaws unfair methods of competition that affect commerce). To address their concerns of competitive suppression and price gouging, the FTC demanded that WCAS permanently halt their add-on deals and undergo “structural relief,” or voiding past transactions to deconstruct the consolidated practices.
PE roll-ups of anesthesia practices have been shown to increase prices by 26% after acquisition.21 In addition, the prevalence of this investment strategy has led PE to control 18.8% of the anesthesia and 22.0% of the emergency medicine market by 2019, representing a sixfold and threefold increase, respectively, in market concentration since 2009.22 As a result, even though high-leverage buyout deals may have been curbed through legislative efforts like the NSA, add-on deals may continue to provide PE with opportunities to obtain rapid returns in healthcare, as this strategy enables them to manipulate natural market dynamics and laws of supply and demand in order to drive up prices and increase profitability.
The FTC’s complaint describes the actions of USAP after its creation. It suggests that USAP is the largest anesthesia practice in Texas, with control over almost 70% of the commercial-insured, hospital-only anesthesia market in Houston and Dallas, and performing almost half of all cases across Texas, while earning nearly 60% of the hospital-only anesthesia revenue. The complaint reports how the firm systematically acquired anesthesia practices within target markets. It also alleges anti-competitive behavior to keep other firms out of the market, and leveraging its billing clout for other anesthesia practices it does not own.23
In May 2024, the court granted WCAS’s motion to dismiss it from the lawsuit, though US Anesthesia Partners’ motion was denied.23 Thus, the ultimate resolution of this question of antitrust enforcement is still unresolved, but WCAS will not be held directly responsible for USAP’s actions. Nevertheless, the negative impact of such consolidations and the financialization of healthcare that results from PE ownership are well-documented, and the future of private capital investment in healthcare needs to be carefully considered while value-decreasing and cost-inflating PE strategies remain lawful.3,24,25
In October 2019, TPG Capital, another leading global PE firm, executed a non-controlling strategic investment in Kelsey-Seybold Clinic Partners, a renowned leader in multispecialty medical group practice management.26
In contrast to the LBO deal type and surprise billing business model deployed by KKR through Envision, the goal of TPG and Kelsey-Seybold’s partnership was two-fold: first, to expand the accountable care model to more geographic locations in the Houston area; and second, to provide additional capital and strategic expertise to the physician leadership who would maintain control of the organization. (Although, TPG quickly flipped the practice to UnitedHealthcare’s Optum in 2022.27 (see related article by Rooke-Ley and Bowling in this issue of HMPI)
This is just one example of how PE has turned its focus to VBC in recent years. According to a 2022 McKinsey analysis, investment activity in companies focused on VBC over patient volume (traditionally seen in fee-for-service or surprise billing models) has increased more than 400% between 2019 and 2021.28 (see study by Nembhard et. al. in this issue of HMPI) Additional examples of recent deals include Kinderhook Industries’ $500 million investment in VBC physician group Physician Partners and the insurance company, Humana’s, $1.2 billion joint venture with Welsh, Carson, Anderson & Stowe to expand the insurer’s VBC clinics for Medicare patients, CenterWell Senior Primary Care.29,30 Similar to TPG’s investment in Kelsey-Seybold, Humana and WCAS aim to scale clinic operations and platform through de novo expansion and inorganic growth.
Analysts largely agree that the growing activity around VBC investments in the private sector is likely driven by concurrent public policy shifts aimed at aligning payor, provider, and investor incentives through improved reimbursement of VBC models.31 However, while these changes may be encouraging, healthy skepticism is still warranted, given the fact that many new VBC systems are just consolidated managed care organizations (MCOs), and thus continue to run the risk of gaining monopolistic market share and pricing power.32
PE’s primary aim of generating returns for investors have often led to tensions between their profit motives and the intrinsic values of the healthcare services they are acquiring and operating, such as accessibility and quality of patient care.25,32,33 Critics argue that the short-term investment horizons of some PE firms may not always align with the long-term nature of healthcare delivery, potentially leading to cost-cutting and profit-maximizing measures that could negatively impact patient care.32,33 In addition, the emphasis on financial performance might overshadow the fundamental healthcare mission of providing patient-centered care. Concerns about PE investment stem from the existing correlations of negative impact on patient care and outcomes with PE acquisition and ownership.25,34
Examples of the historically popular LBO model have not reflected kindly on PE as healthcare systems like Envision Healthcare, Hahnemann Hospital, and Steward Health Care failed to produce the outsized earnings needed to repay their debt and thus faced bankruptcy following PE ownership.19,35–37 (see related Kumar article in this issue of HMPI) The model’s profitability has not only been heavily impacted by regulatory change like the No Surprises Act which removed a key revenue stream—out-of-network surprise billing—but also is subject to significant macroeconomic risk as PE’s ability to repay debt depends heavily on interest rates influencing their cost of capital. An open question, especially from the Steward bankruptcy, is the impact on the community from the financial collapse of an essential public service.24,25
This model has left a great deal of carnage in its wake. In addition to the financial damage to the PE firms themselves from pursuing an unsavory (even unethical) business strategy, there is the loss to the community of the underlying healthcare company, the jobs lost as a result of LBO-induced bankruptcies, and the brunt of the consequences of the business model often manifest as higher prices for patients and worse clinical outcomes due to resource stripping to drive profitability.24,25
While the roll-up model differs from the LBO in its degree of macroeconomic risk, it shares a key question of how PE constructs their core business model. In this case, the concern is that the strategy will use market leverage to drive up prices for services. The USAP case will help define the limits of this strategy and may portend its future application across provider markets.
Finally, the shift in PE add-on focus toward VBC may reflect hope that regulatory and reimbursement model innovation can drive PE cash flows toward delivering greater value to patients. However, as with all roll-ups, PE encounters the same risk of challenges with integration and cost-effective synergy. Furthermore, a common exit strategy is for PE to sell the consolidated outpatient entity to a healthcare services conglomerate, such as Optum, Elevance Health, and CVS Health, which raises further questions about price and quality of clinical services. Physicians and patients may find themselves whipsawed as ownership and governance of practices shift rapidly in the market.
While the cash flows of healthcare delivery remain an attractive target for PE investors, the healthcare system is forced to grapple between the access to capital offered by private investment and the obligation to generate the financial returns required to sustain this investment model. The experience to date of several strategies to solve this equation seem to suggest that we have not yet reached an attractive solution that benefits patients in their search for affordable, high-quality healthcare services. Whether the adoption of “value” as a strategy for the latest round of investments results in a sustainable solution to this challenge remains an open question at this point.
Some observers have recommended policy strategies including improved regulation of fraud and abuse, greater antitrust oversight, regulating price inflation especially with consolidation and roll-ups in areas with limited market competition, and significantly increased transparency in the reporting of PE acquisitions.38 Antitrust enforcement is also a challenge, Currently, only acquisitions over $111.4 million must be reported (under which only 10% PE acquisitions fall), so acquisition of smaller physician practices could easily be missed by antitrust agencies.
There is also concern about the lingering impact of PE investment strategies on cost, quality, and access over time. When individual firms fail, the public must struggle with the fallout. Bankruptcy of PE-backed healthcare firms was the most dominant business failure of any PE-backed sector in 2023.39 The failure of a PE-backed retail chain not only has an impact on employees; it also limits access to essential services for the community. This begs the question of whether the public should be concerned over the long-term impact of PE-investment in healthcare. There is no data yet on what happens to health and healthcare after these bankruptcies. Healthcare providers are a limited resource, and financial distress may motivate early retirement or migration of providers from unstable markets.
As PE focuses more on VBC, many of the top firms ultimately exit their outpatient and specialty care investments by selling to large insurers and their health services branches.27,40 Because regional and services consolidation strengthens these companies’ market power and could lead to higher costs, this strategy could add to the continuously rising cost burden on patients and the entire U.S. healthcare system.40–42
Finally, the challenges of PE investment in healthcare reflect the issue that there is no public agency charged with oversight of healthcare markets in their entirety. There is limited data into the structure of care delivery across markets, and no entity responsible for reviewing this data. The new data transparency requirements may provide some insight into prices across markets and may bring greater visibility to business practices that serve to drive up prices.41 However, these rules still do not extend to many PE-backed practice models.
Lucy W Ma, Stanford University School of Medicine and Graduate School of Business; Shreya A Shah, Stanford University School of Medicine and Graduate School of Business; and Kevin A Schulman, Stanford University School of Medicine and Graduate School of Business, and Clinical Excellence Research Unit, Stanford University School of Medicine
Contact: lucywma@stanford.edu
What is the message?This paper investigates the landscape of private equity (PE) investments in healthcare services over the last decade through a quantitative analysis, exploring how PE investment trends have shifted deal types and sub-sectors. We evaluate the correlation and potential impact of external factors, such as the No Surprises Act and the COVID-19 pandemic, on changing investment strategy. Finally, we explore ways to productively align and synergize PE and healthcare incentives and efforts, as well as highlight the research still needed to continue assessing the true impact of evolving PE activity on patient outcomes and cost burden for individuals and the system.
What is the evidence? The study draws on a comprehensive review of academic literature, industry reports, and investment data from Preqin database to offer insights into the changing patterns of healthcare investments, the strategic focus of PE firms before and after 2020, and the future outlook for key stakeholders within the healthcare sector.
Timeline: Submitted: May 17, 2024; accepted after review May 23, 2024.
Cite as: Lucy W Ma, Shreya A Shah, Kevin A Schulman. 2024. Private Equity Investment Trends in Healthcare: A Decade-Long Review and Quantitative Analysis, 2014 to 2023. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
Private equity (PE) has held a longstanding interest in the healthcare sector, driven by the economic resilience of the sector and its continuous need for capital and innovation. Since the 1980s, PE has gained substantial momentum investing in healthcare services and pharmaceutical companies. For example, an early significant deal in 1989 was a $5.1 billion leveraged buyout (LBO) of Hospital Corporation of America (HCA) by Kohlberg Kravis Roberts (KKR), along with Bain Capital and Merrill Lynch. Over the decade following the 2008 economic crisis, sustained low interest rates significantly boosted PE investment activity not only in healthcare but across various industries.1 However, the healthcare sector saw a disproportionate increase in attention from PE firms due to its stable growth prospects and critical role in society.2
Since the early 2000s, there has been a noticeable shift in the allocation of PE funds within the healthcare services sector, specifically among different types of providers, specialists, and care delivery practices. However, by 2020 there was significant concern about some PE investment strategies in healthcare. One business model that received negative public attention was PE-backed clinical practices that remained out-of-network for health plans, allowing the providers to send exorbitant balance bills charging patients for charges for their services. This practice of “surprise medical bills” led to the enactment of the No Surprises Act (NSA) of 2020, which sought to relieve patients of the financial burden when receiving care without prior informed consent about provider fees.3 Concurrently, 2020 saw the outbreak of the COVID pandemic, causing significant economic distress in the United States, followed by a dramatic rise in interest rates in 2022. As a result, the traditional model of leveraged buyouts (LBOs), which was highly reliant on low rates to refinance debt and often necessitated producing “outsized” earnings to repay immense debt, became less viable. Their notable decline also corresponded with an increase in add-on and roll-up deals, reflecting a strategic pivot towards consolidation and operational improvements in existing companies.
These strategic adjustments highlight the adaptability of PE firms to a changing economic and regulatory environment. The purpose of this paper is to analyze the investment patterns of PE in the healthcare sector, particularly focusing on how deal strategies and target sub-industries have shifted before and after 2020, using comprehensive data from Preqin, the leading database on private investment activity and PE financial data. Through this analysis, we aim to understand the impact of economic and regulatory changes on PE investment behaviors and strategies within the U.S. healthcare landscape.
Dataset
Using data from Prequin, we identified 2,712 PE healthcare deals that had been recorded between January 1, 2014 to December 31, 2023. We first focused on all buyout strategy deals in the timeframe listed above, and included investment deal types including growth, acquisition/buyout, add-on & merger, and other. The “other” category comprised the following deal types: corporate carve out, company formation, joint venture, LP direct, GP stakes, PIPE, private debt, recapitalization, restructuring, and spin-off. Descriptions of the PE’s two primary deal strategies—buyouts and add-ons—and their significance are covered in-depth in the Discussion section. Additional definitions of the other deal strategies included in our dataset can be found in the Appendix (section A.iv). We also included deals with the sectors of Healthcare and Healthcare Specialists listed as the primary industry of the target companies. Finally, we included all deals with the investor and deal locations listed as the United States. We excluded deals that were listed as venture capital strategy, early-stage and late-stage deal types, non-U.S.-based investors or target companies, and had primary industry sectors which were not Healthcare or Healthcare Specialists or were in non-services sectors within the Healthcare category: biopolymers, biotechnology, healthcare IT, medical devices & equipment, and pharmaceuticals.
We also categorized each deal by their sub-industry and specialist service labels in Prequin.
Sub-industries included aesthetic medicine; alternative medicine; clinics/outpatient services; diagnostic, medical & imaging laboratories; emergency services; epidemiology; home healthcare, nursing homes & assisted living; and hospitals.
Specialist services were divided into cardiology; chiropractic; orthopedic & physical therapy; dental products & services; dermatology; healthcare specialists; mental health services; oncology/cancer treatment; and optometrists & opticians products and services.
Analysis
After cleaning the data, we first assessed the descriptive statistics of our data to understand the deal types, sub-industries, and specialists that comprised our included deals. Next, we assessed the number of each deal type that occurred per year. Then we segmented the deal types based on whether it was completed before December 31, 2020 or after January 1, 2020 (pre- vs. post-2020).
Given that we are comparing a seven-year period (pre-2020) and a three-year period (post-2020), we compared the proportions of deals, instead of the raw number, in order to normalize our evaluation of the change in deal types between the two periods. We compared the proportions of each sub-industry and specialist service, among all the deals, on a yearly basis and in the pre- vs. post-2020 periods.
We used Pearson’s chi-squared test to evaluate whether the change in the proportion of deal type, sub-industry, and specialist services was statistically significant between the pre- vs. post-2020 periods. All statistical analyses were performed using R version 2023.12 “Ocean Storm.”
In total, 2,712 unique deals, reflecting 2,821 total deal types, met inclusion criteria for our study (Figure 1). In our cohort, add-on deals were the majority deal type (52%), followed by buyouts (14%) and growth deals (10%) (Table 1a). The median deal size was USD $200 million (interquartile range, IQR $50-700M), and the median enterprise value was $475 million (IQR $120M-1.1B). Deals involving specific sub-industries and specialist services were 71% and 18% of the data, respectively (Table 1b, 1c). Out of the sub-industry deals, nursing homes, clinics/outpatient services, and hospitals were the highest represented categories and had nearly equal proportions (23-24%). Among the deals involving specialist services, mental health services (24%) and dental products and services (24%) comprised the greatest proportion, followed by dental (18%), optometry (16%), and chiropractic and physical therapy practices (15%).
Figure 1 – Flow diagram of deals in study
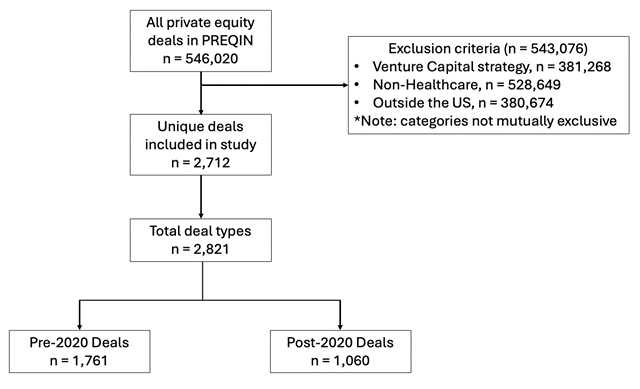
Table 1 – Descriptive statistics of all deals included in study, sorted by: a) deal type, b) sub-industry, c) specialist services
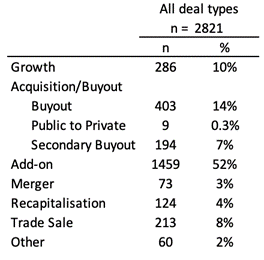
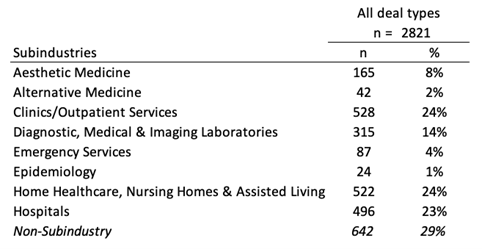
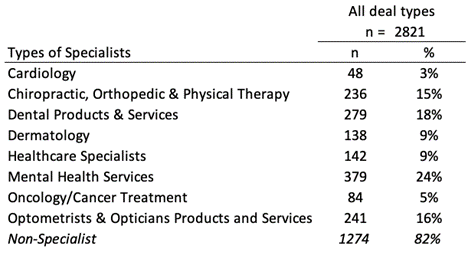
Diving deeper into the deal types, a preliminary analysis of the yearly number of deals by deal type from 2014 to 2023 shows add-ons and buyouts dominating the majority of deals from 2014 to 2020 (Figure 2). Growth drivers of healthcare investments since 2014 included a robust stock market, which increased access to capital and enabled higher company valuations attracting PE investment activity; low interest rates, which reduced cost of debt and decreased financing risk, also enabling investments; the passage of the Affordable Care Act in 2010 driving healthcare reform and consolidation as it promoted pay-for-value over pay-for-volume reimbursement models; Trump’s election and his administration’s business-friendly policies which boosted M&A activity; and the COVID-19 pandemic which accelerated digital health solutions, telemedicine, and overall healthcare delivery expansion and opportunity to break into new geographic sectors and markets..4,5 Around this point, we see a massive rise in add-ons from 2020 to 2021 and then a gradual leveling out back to its previous baseline seen during 2018 to 2020 (Figure 2, purple curve). In contrast, buyouts demonstrate a steady drop-off in 2018 and then again in 2021 through 2023 (Figure 2, orange curve).
Figure 2 – Change in number of each deal type by year from 2014-2023
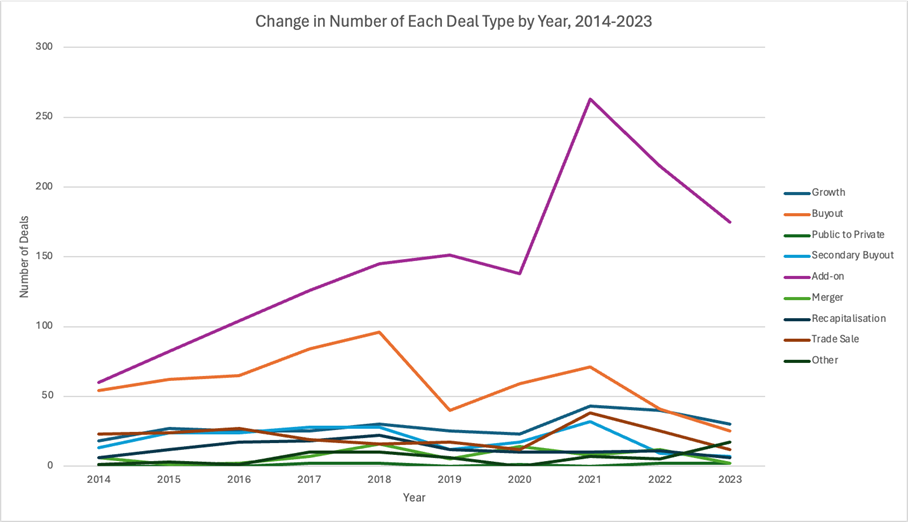
Segmenting the deal types into pre- and post-2020 periods, we initially observe that add-ons consistently represented a significant portion of all deal types in both periods, with buyouts and growth deals following behind (Table 2). While growth, privatization, merger, and other deals account for relatively similar proportions of pre- and post-2020 deal types, there were notable changes in buyout, secondary buyout, add-on, and recapitalization deals, particularly in their proportions between the two periods (-53%, -45%, +35%, and -54% change in proportions, respectively; p < 0.001 for all comparisons).
Furthermore, within sub-industry deals between pre- and post-2020, we found statistically significant decreases in PE investment in aesthetic medicine (-33%), emergency medicine (-47%;), epidemiology (-79%), and hospitals (-43%), as well as a significant increase in clinics/outpatient services (+117%) (p < 0.05 for all). Finally, among the deals involving specialist services, we determined there was a statistically significant increase in PE investment into cardiology (+185%), chiropractic and physical therapy (+89%), and other specialist practices (+139%) and a statistically significant decrease in mental health service (-19%) and optometry practice investments (-11%) (p < 0.05 for all). The yearly number of deals by sub-industry and specialist service can be found in the Appendix (Table A.i-iii, Figure A.i-ii)
Table 2 – Deal types, sub-industries, and specialists by pre- and post-2020 period
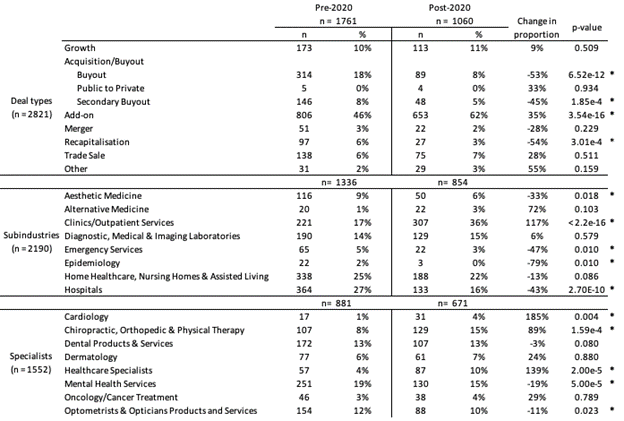
Healthcare has historically represented an attractive investment opportunity for PE due to its recession-resilient economic growth, legislative efforts to encourage innovation, and growing need for capital. In particular, since the 2008 economic crisis, a consistent slough of years with low interest rates under 3% have drastically increased PE’s investment activity across the board (Figure 3).6,7 Total capital invested by PE has increased as interest rates have dropped, reflecting an inverse correlation of capital invested and Fed rate.6 Of note, over this period, PE firms shifted a greater proportion of their investment funds toward healthcare and away from other sectors. For instance, the proportion of PE capital invested in healthcare leveraged buyouts (LBO) shifted from less than 5% of all LBO funds in 2000 to 14% in 2018.7
In this study, we sought to examine the types of deals that characterized healthcare PE investment over the past decade. Given the lack of transparency and data around PE activity in the healthcare sector, we aimed to better characterize their investment choices.8
Since the 1980s, the most common financing model used by PE in healthcare has been an LBO, in which a PE firm uses a significant amount of borrowed money to buy a majority stake in a healthcare company. The buyout targets of these transactions tend to be healthcare companies with strong stable cash flows and opportunity for potential operational improvements to generate high enough earnings to repay the debt used to acquire the company. Debt can represent a significant portion of payment for the target, sometimes as high as 70%7. The ultimate goal of many LBOs is to sell the acquired company at a higher value than its purchase price, such as to another PE firm, a public offering, or another company.5,7,9
Another investment model is the “platform and add-on” or “add-on and merger” approach, which aims to build value through consolidation of smaller companies into a platform, or a larger, core company.10 Also called “buy and build”, this strategy seeks to create value through synergy, economies of scale, and in some cases, care coordination to address patients’ diverse needs.2 The platform company typically has substantial market share, financial stability, and a scalable business model to integrate “add-on” acquisitions effectively. These add-ons are smaller companies that are integrated into the platform to drive growth, achieve cost efficiencies, diversify services offerings (such as different clinical specialties), or expand market share (which often also increases the PE ownership and platform company’s pricing power or negotiating power with payers).11
In our data analysis, we found a stark drop in buyout deal types after 2020, including secondary buyouts.7 Add-on deals increased in proportion by 35%, accounting for a majority of PE deals in the post-2020 period. Furthermore, the total deal value in healthcare dropped significantly from $151 billion in 2021 to $90 billion in 2022.4,5
Our finding of the decrease in healthcare investments, in particular LBOs, likely converges with two macroeconomic factors. First, as U.S. economic activity recovered after the pandemic, interest rates have increased to multi-decade highs, which means PE funds operating highly leveraged buyouts can no longer depend on a low cost of debt and higher valuations to turn a profit.6 Healthcare deals were very heavily funded by debt, which could include debt multiples of 11x despite Federal Accounting Standards Board recommendations that banks do not loan more than 6x EBITDA.5,12 As a result, investors needed to focus more on actual revenue growth strategy and operational improvements to meet their expected returns. Second, the passage of the No Surprises Act (NSA) in 2020 restricted PE firms from investing in LBOs providing out-of-network healthcare services and then implementing a business model of surprise (balance) billing.3,13,14
In addition to these two major considerations, we recognize other significant concurrent factors that contributed to decreased investments, including negative sentiment and growing criticism, tightening of labor markets necessitating higher wages, instability among banks which restricted financing deals over $1 billion, as well as a growing number of PE firms seeking to directly partner with hospitals, all of which changed PE’s investment foci and activity across the healthcare industry.4
Given the increase in the cost of debt and the limits in revenue resulting from the NSA, PE firms found that they could no longer continue LBOs. Conducting such highly leveraged deals placed excess pressure on PE firms to extract outsized earnings from their deals, a goal that drove incentive misalignment in healthcare, negatively impacting physicians and patients.5,7
Further insight into the influence of the NSA on PE investment activity comes from analyzing the sub-industry and specialist trends. Aesthetic medicine, emergency medicine, and hospitals were all high targets of PE investment because elective medicine tended to be out-of-network, emergency medicine could also be out-of-network (a big focus in roll-ups and surprise billing15–17), and hospitals could be obtained in LBOs and their assets used as collateral for loans. As a result, the correlation of the decline in these three sub-industries with the passage of the NSA in 2020 appears consistent with the logic that the NSA disrupted these sectors’ reliable profitability for PE in the setting of LBOs and investors have shifted their primary focus away from this strategy, at least for now.
Since 2020, we observe a dramatic rise in clinics and outpatient services from 17% to 36%, a statistically significant 117% increase that may be part of PE’s growing shift toward add-on deals. Add-ons are an effective way for PE firms to gain market share and pricing power through consolidation of local and regional players, and PE has traditionally implemented this deal type in anesthesiology and emergency medicine.18 However, with the rise in value-based care (VBC) reimbursement models, PE seems to be following the tides of regulatory shifts, away from LBOs of out-of-network practices and surprise billing, and toward consolidation of specialist outpatient clinics. In fact, PE investment activity in companies focused on VBC over patient volume (traditionally seen in surprise billing models) has increased more than 400% between 2019 and 2021 according to a 2022 McKinsey report.19
Surprisingly, we had expected to observe a much more significant increase in PE investment toward imaging laboratories and decrease in investment toward nursing homes pre- and post-2020 because of the profitability of radiology services (due to increasing technology and imaging usage in medical standard of care, as well as reliably high patient throughput) and the negative outcomes seen in PE-owned nursing homes, respectively.20,21 However, our analysis showed that investment in both of these sub-industries stayed relatively constant before and after 2020, with only a 1% increase in the proportion of laboratory service investments and a slight decrease in the proportion of nursing homes out of all PE healthcare investments. We hypothesize that PE’s stagnant interest in radiology services, compared to rising activity involving clinics and outpatient services, likely derives from shifting reimbursement trends in the market.
Another possible hypothesis is that PE’s motivation to acquire clinics followed the boom in large retailers’ consolidation of physician practices. As big-box retailers and pharmacy chains like Walmart, CVS Health, and Walgreens sought to create integrated care networks and leverage market power, PE likely identified a key opportunity in improving or consolidating previously fragmented primary care physicians and other specialist practices in key geographies or markets and selling them as strategic add-ons. The most prominent examples include the acquisition of practices by firms like One Medical, Iora Health, and Oak Street Health, with peak investment years around 2017 and 2018, and the eventual acquisition of these companies by the aforementioned big-box retailers and pharmacy chains: Amazon and One Medical, CVS and Oak Street Health.4,22–24 Further research and analysis is needed to fully examine the nature of these relationships and the impacts of these retailer acquisitions on patient outcomes and healthcare costs.
The critical question that has been raised in the healthcare PE setting is whether the incentives of funds driven by short-horizon, high-percent ROI can truly be aligned with the needs for improved longitudinal patient outcomes and sustainability of a high-quality care delivery system. We believe that public policies like the No Surprises Act are critical guardrails to prevent adverse strategies by powerful financial entities that can destabilize, even lead to the collapse of, existing healthcare systems.25 However, punitive or restrictive measures alone are not enough; policy that positively reinforces improving sustainability, enhancing quality of care, and decreasing costs is just as important. Finally, continuing research needs to examine how PE ownership might affect outcomes of patients cared for by their portfolio companies.
As with any retrospective study, our work has limitations to address. First, our data on PE investments was limited to Preqin, public news articles, and press releases. As a result, there may be a few deals missing from our time period if they were not publicly released or recorded in Preqin. However, given that Preqin is the leading source for private investing activity, we chose to utilize Preqin data over Pitchbook because of the high quality of the database and the ability to conduct much more in-depth and rigorous data analysis external to the platform.
Second, our study’s outcome of interest—change in investment deals pre- and post-2020—is a transition point that marks several significant events, from the NSA to the COVID-19 pandemic to significant macroeconomic factors. As a result, we are not able to fully disentangle the impact that each factor might have had on our analysis. Given the complex landscape of the healthcare industry, we readily acknowledge that all these aspects contributed to the changes we observe in PE investment trends.
Finally, underreporting of PE investments, in particular smaller deal sizes and enterprise values, is a well-known occurrence and limitation of all private finance databases.8 There may be a higher number of PE deals over the last ten years than those included, likely with lower valuations since only acquisitions over $111.4 million must be reported. Nevertheless, Preqin is the most comprehensive database on the private investments that we can readily download and process with more sophisticated data analysis tools, which provides quantitative rigor and critical insight into the factors that we evaluated for association with our outcomes of interest.
References
Appendix
Table A.i – Change in number of each deal type, year on year, 2014-2023 (correlates with Fig 2)
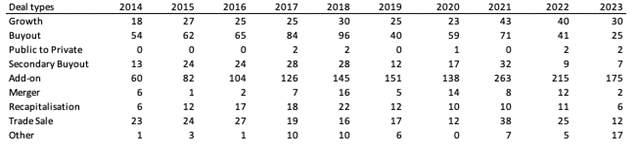
Table A.ii – Change in number of sub-industry deals, year on year, 2014-2023
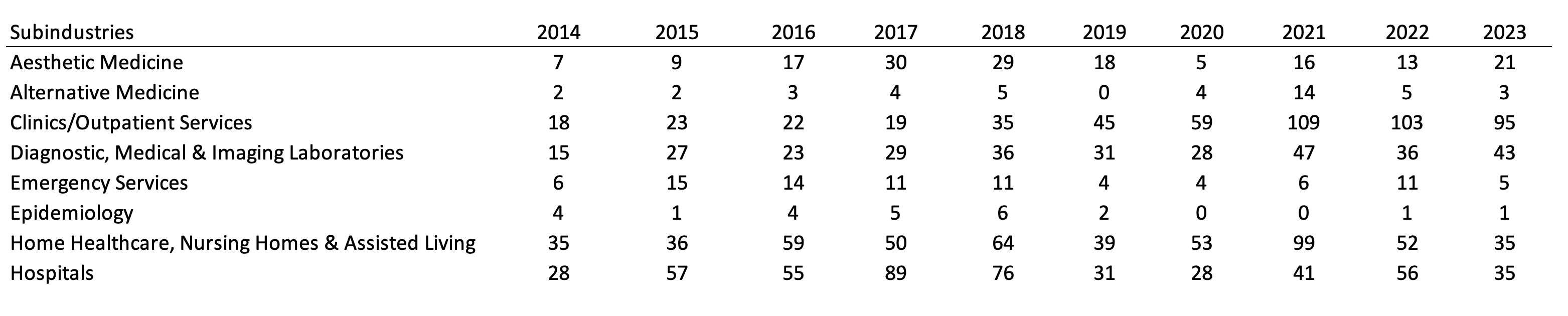
Figure A.i – Change in number of sub-industry deals, year on year, 2014-2023
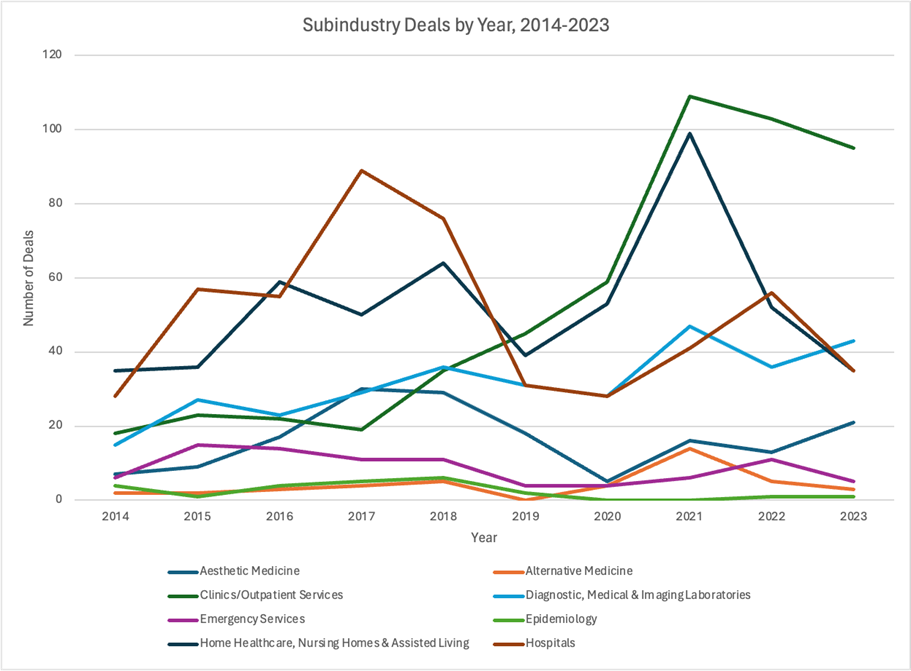
Table A.iii – Change in number of specialist deals, year on year, 2014-2023
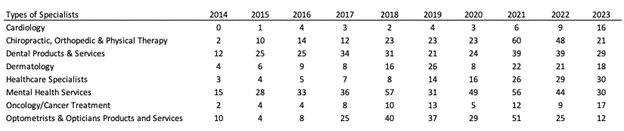
Figure A.ii – Change in number of specialist deals, year on year, 2014-2023
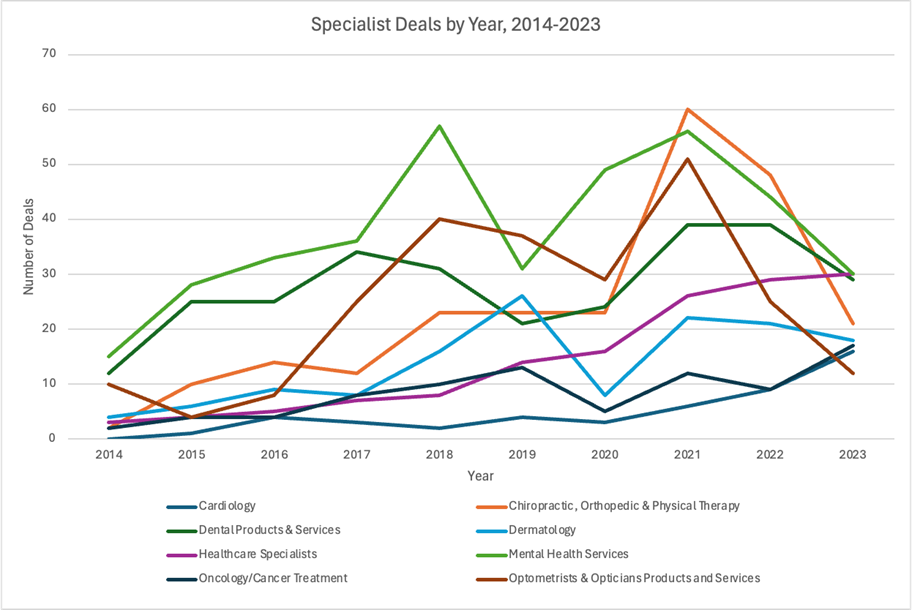
A.iv Definitions of “Other” Deal Types
Oluwatobi (Tobi) Ogbechie-Godec, APDerm
Contact: taogbechie@gmail.com
What is the message? The goal of physician leaders in healthcare should be to improve the health of the population while providing a sustainable and fulfilling career for the clinicians and clinical support staff in a practice. The exponential increases in the spending to deliver healthcare has fueled the disruptive forces that are primarily aimed to increase scale, not necessarily to improve the health and wellness of patients, clinicians, and clinical support staff. This current state presents an opportunity for physician leaders in healthcare management.
What is the evidence? Over the last decades, private equity involvement in healthcare delivery and clinical practices has increased. While there is evidence demonstrating some negative outcomes in specific circumstances, it is important to understand the drivers of these negative outcomes in patient out-of-pocket costs, increased prices to payers, and health outcomes. The leadership and management structures of all healthcare institutions are likely to play a larger role in driving these outcomes, rather than the financial model itself.
Timeline: Submitted: April 22, 2024; accepted after review June 12, 2024.
Cite as: Oluwatobi Ogbechie-Godec. 2024. Opportunity or Cost: Physician Leaders in Private Equity. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
At a recent gathering of prior joint-degree graduates from both the medical and business schools at my alma matter, I was struck by the message from the keynote speaker. The intimate gathering was the largest gathering that I had ever attended of MD/MBAs. The typical path of an MD/MBA graduate was to choose one of two paths – we either remained strictly clinical or crossed over to the other side to become mostly managers. However, in this setting, we had multiple joint degree graduates who had continued clinical practice while taking on leadership and managerial roles in our various organizations. The keynote speaker began his speech laying out the current issues in healthcare – ever increasing spending in healthcare, concerning burnout among clinicians and clinical support staff, plateauing clinical outcomes for chronic health conditions, patient frustration with the complexities of the system, and lack of improvement in various health equity indicators. As he continued on, I was awaiting his message for hope of change. I eagerly listened for the punch line where he would announce that physician managers had already begun cracking this code and reversing these trends. In this room, we had physician financial investors, physician chief executives of large companies, physician leaders of large healthcare networks, and physician leaders in academia. Surely, one of us would be commended for solving this enigma. However, the punch line in his speech never came. Were we all complicit in maintaining the status quo?
I was one of those physician executives in the audience. Since college, I have always been fascinated by the interplay of medicine and management after a personal experience led me to understand that the healthcare I received was at the end of the delivery chain – long after the succession of decisions by others who were not in the exam room. In my operations courses in business school, I remember learning about how managers were able to optimize performance on the production line (Spear & Bowen). It struck me that all levels of management of this manufacturing facility had a good understanding of what the functionality and quality of the final product should be, and thus, they were agile in responding to production challenges. From my experiences and education, I was convinced that most managers of healthcare practices and institutions did not have a complete understanding of the complexities of healthcare delivery. In many ways, that is because of the complexity of the system. My goal was to bring my knowledge of the clinical scenarios, coding and reimbursement, patient behaviors, and clinical outcomes into consideration for decisions that are made by the leadership of healthcare practices. When classmates and other physicians would ask me about why I was enrolled in a joint degree program for medicine and business, I would respond that I saw myself as a Trojan Horse bringing clinical knowledge into the decision rooms.
After a decade, I am now in my current role as a Chief Medical Officer at a dermatology and plastic surgery group, a growing practice with about 100 clinicians. In this role, I work with the management teams on various operational, financial, and clinical initiatives. A critical component of my role is that I still see patients. I have maintained a general practice where I see patients of all types for medical, surgical, and cosmetic dermatology. Not only does my clinical practice allow me to understand the consequences of the policies, procedures, and technologies that we implement, but it also provides comfort to the practicing clinicians and the clinical staff to know that they have representation at the decision table. The non-clinical leadership team is also very receptive to having a physician on the leadership team. During our discussions, I learn as much from them as they do from me when we debate important issues that affect our clinic operations. This partnership has been very fulfilling as we have grown our clinical volume tremendously during my time in this company. Overall, I never needed to be a Trojan Horse in my current practice because my insights were welcomed in the discussions and decision-making. Some may be surprised that my practice is affiliated with private equity investments, but I am not.
Consolidation has been the big theme in healthcare in recent decades (Moses, et al., 2013). Over time, other private payers have increasingly become more consolidated (Robinson, 2004) (Levinson, Godwin, Hulver, & and Neuman, 2024). Clinicians have responded by similarly consolidating to enable scale for purchasing power, payer negotiations, and patient coordination (Kimmey, et al., 2021). In fact, there has been consolidation at all levels of healthcare delivery – clinic supplies, pharmaceuticals, medical equipment, technology and applications, health information exchange networks, etc. There has been both vertical and horizontal integration and consolidation. Moreover the complexity of the administrative burden in healthcare has increased (Zegers, et al., 2022). These forces are powerful and have promoted the entry of third-party solutions that aim to simply the complexity primarily for one stakeholder in the delivery chain, while furthering the complexity for all the others. This consolidation was occurring even before private equity growth in healthcare (David, Simon, & White, 2002).
I witness the effects of the healthcare delivery complexity daily in my clinic. A recent patient interaction highlighted the effects of the presence of all these misaligned stakeholders in healthcare delivery. A young woman came to see me for treatment of her worsening psoriasis. She had been diagnosed with psoriasis for over a decade but was never able to obtain consistent treatment due to periods of uninsurance as she changed employment. When she was finally consistently insured, she was covered under the state Medicaid plan which most private practice dermatologists do not take due to severe underpayment and other administrative burdens. She now transitioned into a managed care plan, which few private practice dermatologists accept. Upon clinical presentation, she had over 15% of her body surface area covered in psoriatic plaques. Due to her skin color, there was an additional 20% of her body surface area with dark patches, post-inflammatory hyperpigmentation, which stemmed from the lingering effect of the psoriasis after inflammation. The main reason why she presented to me was that the itching had become unbearable, and it kept her up at night. To prescribe a biologic medication that was both safe and effective for her, I had her fill out a patient assistance form while in clinic since many patients need some financial assistance to obtain the drug. I prescribed the medication to a national pharmacy that offers a solution to larger practices to perform prior authorizations, which saves time for our clinical staff. The patient’s insurance responded that the biologic medication was a non-covered drug on her plan, thus she was underinsured. Several members of my team spent about three cumulative hours on the phone with numerous electronic health record messages that became increasingly difficult to follow. They were eventually able to get her coverage for the drug through the pharmaceutical company based on compassionate care. This level of effort for one episode of care for one patient is not sustainable. A major reason why it was possible was that I was part of a consolidated dermatology practice that was able to absorb the low reimbursement by her managed care plan, create centralized prior authorization departments, and forge partnerships with larger national pharmaceutical companies and pharmacy chains. This would neither be possible in a smaller practice due to limited resources, nor in a larger multispecialty or academic group as dermatology operations would not be prioritized over primary care or higher spending specialties.
It is worth noting that I played an instrumental role in forging those partnerships with the national pharmaceutical companies and pharmacy chains because I understood the needs and frustrations of my clinical teams. Their frustrations are my frustrations. Overall, the status quo is not sustainable for patients and clinicians.
In my current role, I am constantly solicited by third parties about solutions for scheduling, patient communications, patient access, marketing, among others. Their pitch is often that they are ‘the’ innovative solution to make my company operate more efficiently. Few of them are truly innovative; instead, they are hoping to replace personnel in the company. Most of the innovative companies face hurdles to fit into the already complex web of the healthcare delivery system. For example, a patient communication platform must seamlessly integrate with the practice management system for scheduling, the billing system (internal and third party), the electronic medical record, and the post-visit patient communication system. Any deficit in the integration will create more layers of complexity and additional resources to patch the inadequate interface. For example, if the system does not integrate well with the electronic medical record, clinicians and clinical support staff would need to create accessory pathways or workarounds to reconcile the patient’s messages with information that is accessible at the time of the visit.
Technological innovation in health delivery is stymied by the lack of interoperability, transparency, accountability, and reward. Healthcare delivery system innovation is equally hampered by the need for scale and the unclear reward system. Certain delivery models are inherently fraught with tension – value-based care delivery models are inevitably going to decrease spending by eliminating or reducing the earnings of one or more players in the delivery chain. Even notable technology, logistics, and finance entrants into healthcare delivery have not garnered as much success as was initially envisioned (Hensley, n.d.). It appears that disruptive innovation in healthcare is extremely difficult to attain (Hwang & Christensen, 2008).
I remember when I was interviewing to be a physician manager in various healthcare delivery settings. While I considered multiple roles, I distinctively remember two roles – one in an academic center, the other at a physician-owned private practice. An academic center was going to appoint me to a “quality” role, which was intended to be a stepping stone into hospital administration leadership. I was explicitly warned that the path to becoming a key decision maker meant waiting for the current leaders to decide to retire or move on. Furthermore, a major requirement of the role would be research. I probed the team on why research was necessary for an operational and managerial role, but the answer I was given was not satisfactory to me. At another interview with a physician-owned large private practice, I was welcomed to participate in the management of the practice and to lead growth initiatives. However, the only caveat was that I had to do it on my own time without any explicit compensation. Partnership would be discussed after two years. Roles where I would have more management duties would likely affect my clinical practice, which I thought was crucial to being a physician leader.
After much deliberation with mentors, coaches, colleagues, and family, I accepted the role at my current company, where I am both a clinician and an executive who sets the clinical strategy and quality goals. What drew me to the company were the people, the excellent reputation, the explicit promise of high-quality dermatologic care, and the embedded structure of physician leadership. In some circles, private equity affiliated practices are often accused of placing profit over clinical care. However, the freedom of the management structure encourages efficiency and creativity in the clinic and hospital setting. The structure also encourages innovators in other fields to engage in healthcare by providing accessible incentives in the complex healthcare landscape. To be a sustainable healthcare company, one must prioritize patient outcomes, patient experiences, clinicians’ satisfaction, and teammate satisfaction.
Since joining, I have worked with the management team on multiple projects to create accountability for patient access with the call centers, improve the success of electronic health record implementations by ensuring that clinical workflow designs are captured in the initial launch; improve efficiency of the prior authorization process by understanding which portions of the workflow can be outsourced to an external party; improve the hiring and training processes of clinical staff to enable continued clinician productivity; increase accountability in the revenue cycle and billing departments to understand how to efficiently capture value for the work that the clinicians are already performing; engage payers to educate them about the value of community dermatologists; and much more. compared with other dermatology practices. Our team was much more nimble during the COVID-19 pandemic, resuming patient care within one to three weeks after the March 2020 shutdown. We were able to get back to scale much faster than the dermatologists in academic or multispecialty groups since we were much more agile.
Anecdotally, my experiences may be different from some other private equity-affiliated dermatology groups. Some of the dermatologists in these other groups complain about productivity quotas being placed on them that do not account for the clinician’s skill or a patient’s complexity. Other groups have put in place cost-saving but burdensome systems, such as eliminating a clinical triage team and passing all patient messages directly to the clinicians. This practice contributes to physician burnout (Ratanawongsa, et al., 2008). Research has also shown that private equity affiliates may result in increases in a patient’s costs and the share of non-physician clinicians in the practice (Bruch, 2023) (Singh Y, 2022). A common theme that I see in these other private equity models is that there is an explicit lack of a physician leader in the group’s decision-making room. We need more insight into understanding the impact of the leadership team on the critical measures and key indicators of a successful healthcare delivery system.
Private equity affiliations enable healthcare practices to scale, and they provide managerial flexibility to innovate. Whether healthcare delivery systems choose to capitalize on that opportunity is up to the leaders of the delivery system – in particular, the presence of a strong physician leader is crucial to understanding whether the practice will focus on any of the quintuple aims of healthcare delivery (Nundy S, 2022).
Overall, I do not regularly think about my company’s affiliation with private equity. I am grateful for the opportunity to provide access to patients who would otherwise be underserved because of the scale that we have created.
I think back to the keynote speech at the joint degree gathering of MD/MBA alumna. While I will never know the speaker’s intentions of his address on the misaligned incentives and the resulting issues in the U.S. healthcare delivery system, I choose to see his speech as a call to action. It is a call to action to the physician leaders who are in positions where they do not have the ability to use their training and clinical expertise to change the system from within. We need more physician leaders who still practice clinically within the systems that they lead. With this, some of them will truly be able to capitalize on opportunities to innovate and improve the health and wellness of our patients and our clinical teams.
References
David, D., Simon, C. J., & White, W. D. (2002). Is Managed Care Leading to Consolidation in Health-care Markets? Health Services Research, 37(3), 573-594. Retrieved 4 21, 2024, from https://ncbi.nlm.nih.gov/pmc/articles/pmc1434652
Hensley, S. (n.d.). Atul Gawande Named CEO Of Health Venture By Amazon, Berkshire Hathaway And JPMorgan. Retrieved 4 21, 2024, from https://www.npr.org/sections/health-shots/2018/06/20/621808003/atul-gawande-named-ceo-of-health-venture-by-amazon-berkshire-hathaway-and-jpmorg
Hwang, J., & Christensen, C. M. (2008). Disruptive Innovation In Health Care Delivery: A Framework For Business-Model Innovation. Health Affairs, 27(5), 1329-1335. Retrieved 4 21, 2024, from https://healthaffairs.org/doi/full/10.1377/hlthaff.27.5.1329
Kimmey, L., Furukawa, M., Jones, D., RM, M., J, G., & EC, R. (2021, Jan). Geographic Variation In The Consolidation Of Physicians Into Health Systems, 2016-18. Health Aff (Millwood), 40(1), 165-169. doi:10.1377/hlthaff.2020.00812
Levinson, Z., Godwin, J., Hulver, S., & and Neuman, T. (2024, Apr 19). Ten Things to Know About Consolidation in Health Care Provider Markets. Retrieved from KFF: https://www.kff.org/health-costs/issue-brief/ten-things-to-know-about-consolidation-in-health-care-provider-markets/#:~:text=Consolidation%20in%20health%20care%20markets%20can%20take%20many%20forms%20and,mergers%E2%80%9D%20in%20this%20brief).
Moses, H., Matheson, D. H., Dorsey, E. R., Dorsey, E. R., George, B. P., Sadoff, D., & Yoshimura, S. (2013). The Anatomy of Health Care in the United States. JAMA, 310(18), 1947-1964. Retrieved 4 21, 2024, from https://jamanetwork.com/journals/jama/fullarticle/1769890
Ogbechie-Godec, O. A., Mostaghimi, A., & Nambudiri, V. E. (2018). Skin in the Game: Existing and Upcoming Physician Payment Models in Dermatology. Journal of The American Academy of Dermatology, 79(1), 175-177. Retrieved 4 21, 2024, from https://jaad.org/article/s0190-9622(18)30151-8/fulltext
Ratanawongsa, N., Roter, D., MC, B., SL, L., SM, L., KA, C., & LA, C. (2008, Oct). Physician burnout and patient-physician communication during primary care encounters. J Gen Intern Med, 23(10). doi:10.1007/s11606-008-0702-1
Robinson, J. C. (2004). Consolidation And The Transformation Of Competition In Health Insurance. Health Affairs, 23(6), 11-24. Retrieved 4 21, 2024, from https://healthaffairs.org/doi/full/10.1377/hlthaff.23.6.11
Spear, S., & Bowen, H. K. (n.d.). Decoding the DNA of the Toyota Production System. Harvard Business Review. Retrieved 4 21, 2024, from http://hbr.org/1999/09/decoding-the-dna-of-the-toyota-production-system/ar/1
Zegers, M., GL, V., G, G., R, V., HJG, v. d., & GA, W. (2022). Perceived Burden Due to Registrations for Quality Monitoring and Improvement in Hospitals: A Mixed Methods Study. Int J Health Policy Manag, 11(2), 183-196. doi:10.34172/ijhpm.2020.96
Hayden Rooke-Ley, American Economic Liberties Project, and Daniel S. Bowling, Georgia State University
Contact: hayden.k.rookeley@gmail.com
What is the message? As the corporatization of the medical profession continues, physicians are increasingly turning to labor law to collectively bargain over the terms and conditions of their employment. However, due to state bans on the corporate practice of medicine (CPOM), physicians working for private-equity-backed companies, hospitals, and other corporations are often not directly employed by these corporate entities. Such complex and indirect employment arrangements heighten the salience of labor law doctrines that, at times, allow unionized workers to compel multiple corporate entities to collectively bargain, including those that do not directly employ the workers. As physicians unionize, legal disputes over the application of these doctrines are beginning to surface and may shape the contours of physician unionization and CPOM bans.
What is the evidence? A review and analysis of recent labor law, legislative initiatives, court rulings, legal doctrine, and market developments.
Timeline: Submitted: May 24, 2024; accepted after review May 29, 2024.
Cite as: Hayden Rooke-Ley, Daniel S. Bowling. 2024. Controlled But Not Employed: The Clash of Labor Law and the Corporate Practice of Medicine. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
Physicians are beginning to unionize in response to increasing corporate employment. However, these employment relationships are often indirect and complex, involving numerous corporate entities that jointly exercise control over physicians. In fact, due largely to state bans on the corporate practice of medicine (CPOM), many hospitals and corporate-owned medical practices do not actually employ physicians. Such arrangements raise the salience of two related law labor law doctrines: the “single employer doctrine” and the “joint employer doctrine.” Both doctrines can enable employees to unionize against non-employer entities that nonetheless control their working conditions. As discussed below, the application of these doctrines, which is now beginning to occur, may shape the contours of physician unionization and CPOM enforcement.
The current corporate structures of physician employment formed in response to state bans on the corporate practice of medicine (CPOM). Historically, these bans prohibited corporate entities from owning, controlling, or employing physicians.[1] Rising to prominence in the mid-1900s, these laws often originated in state courts through judge-made or “common” law. State legislators followed suit, codifying CPOM bans by prohibiting lay entities from clinical decision-making and requiring for-profit medical practices to be physician-owned.
While states have relaxed CPOM enforcement since the 1970s, the basic structure of these laws is largely still in place: medical practices must be exclusively or majority owned by licensed clinicians, typically physicians. And as corporatization of the medical sector continues, numerous states are now looking to strengthen these laws.[2] Due to this legal ownership landscape, corporations interested in controlling the medical practice have devised a workaround, known as the “PC-MSO,” or “Friendly PC” model (“PC” stands for “professional corporation,” which is a common corporate form of physician-owned medical practices). In these arrangements, a corporate entity, such as a private-equity-backed company, will use the vehicle of a management services organization (MSO) to exercise functional control over a medical practice or a physician staffing company.
While MSOs traditionally assist medical practices with back-office administrative tasks, lay-owned corporations – through contracting – can transform the MSO into the controlling entity. For example, the MSO often takes control of all business and administrative elements of the practice, allowing it to require that physicians see more patients, dictate coding and billing procedures, make personnel and scheduling decisions, and control many of their functions of the practice that influence the nature and quality of care delivered. MSOs may also require that physicians sign restrictive contracts such as noncompete agreements, gag clauses, and stock transfer restriction agreements (STRAs), which in effect place the MSO in control of the equity of the physicians.
In the most extreme version, the Friendly PC model, the MSO will install a “friendly” or “captive” physician leader. This physician will be licensed in the state to practice medicine and can therefore satisfy the formal requirements of physician ownership, but in substance, the physician serves as a direct extension of the MSO. This physician, who may not actually practice at the clinic, is often financially compensated by the MSO and even serves on its executive board. The physician may have a direct role in MSO management or receive a minority equity stake in the MSO.
Another scenario of corporate non-employer control implicates hospitals. Many hospital-based physicians work for a corporate staffing company that contracts on behalf of physicians with the hospital. This practice, too, has historical roots in CPOM laws, which barred hospitals from employing physicians. That prohibition continues in some states today, such as Texas and California. The use of physician staffing companies is pervasive even in states that permit direct employment by hospitals. In these arrangements, the hospital, as a party to the contract with the staffing company, exercises varying degrees of control over the employed physicians. Like MSOs in the PC-MSO context, however, the hospital entity is not the formal employer of the physician (nor might be the staffing company using the PC-MSO model).
The upshot of these arrangements is that the corporate entity exercising control of physicians is not actually the legal employer. As physicians are increasingly attempting to unionize under these structures, the fact that the corporation is not the physicians’ employer complicates the application of federal labor law, which is largely predicated upon a direct employer-employee relationship.
Under the National Labor Relations Act (NLRA), which governs private-sector unions, only “employees” can organize a union, and independent contractors are expressly excluded. The NLRA defines neither employees nor independent contractors, so issues regarding employee eligibility have been the subject of litigation for decades. The NLRA also only references “employers,” which typically involves a single employer. But as corporate ownership structures have become more complex, the National Labor Relations Board (NLRB) has developed two related doctrines that, at times, can broaden the NLRA’s scope to include corporate entities that are not technically employers but functionally operate as such.
The first of these doctrines is the “single employer” doctrine. It applies in situations where there appears to be multiple entities controlling the employees, yet they functionally operate as one enterprise so that “for all purposes, there is in fact only a single employer.”[3] If the entities are deemed a single employer, the NLRA’s protections for collective bargaining apply to it as if it were one employer, rather than multiple separate entities. To determine whether these multiple entities constitute a single employer, the NLRB looks at whether there is interrelation of operations, centralized control of labor relations, common management, and common ownership or financial control.[4] Centralized control over labor relations tends to be the most critical element, and common ownership, while typically necessary, is not dispositive. The single employer doctrine tends to be used in the context of a business subcontracting integral parts of its operations.
A related but distinct principle of labor law is the joint employer doctrine, which has been subject to significant legal disputes in recent years. Historically, courts and the NLRB found joint employment where one or more entities exert “direct and immediate” control over the employment terms of employees seeking unionization. Under this fact-specific inquiry, if a group of employees can show that an entity effectively controls the working conditions of unionizing employees, it will be found to be a joint employer with the direct employer and compelled to comply with the requirements of labor law, such as good-faith collective bargaining.
In 2015, the NLRB relaxed the “direct and immediate” standard for the joint employer doctrine in Browning-Ferris Industries, which held that the putative joint employer need only “share or codetermine” the terms and conditions of employment.[5] The ruling implicated businesses that make heavy use of contractors, staffing companies, and franchisors, and drew vigorous opposition from the Chamber of Commerce and employers such as McDonald’s.[6] The Trump Administration’s pro-business NLRB then issued regulations in 2020 returning the standard to the pre-Browning “direct and immediate” control requirement. Later in 2023, the Biden NLRB issued yet another set of rules discarding the 2020 rules and reimplementing the Browning-Ferris standard, but a U.S. District Court promptly stayed the new rules’ enforcement, a ruling that is now pending appeal.[7] Going forward, the standard will remain subject to much dispute, and it may influence the outcome of joint-employer questions in the context of physician unionization.
Whether physicians can successfully invoke the single and joint employer doctrines will influence the effectiveness of unionization. For example, if physicians unionize against a staffing company but are unable to compel a hospital to collectively bargain, the physicians will be unable to negotiate working conditions dictated by the hospitals. The same is true for physicians employed under a PC-MSO structure: the MSO, if it can avoid the status of employer, would not be compelled to bargain over the working conditions it controls. On the other hand, if physicians can invoke these doctrines, they will not only be able to bargain over all the conditions of their employment; they’ll also be protected from retaliation for unionizing or striking, as labor law would prohibit the hospital, for example, from terminating a contract with a physician staffing company in response to unionization.
These labor law questions could also implicate the enforcement of CPOM bans. In states where CPOM bans prohibit corporate employment of physicians, findings from the NLRB and courts that MSOs or hospitals are essentially functioning as employers could encourage tighter regulation of the PC-MSO model. The specter of such findings could serve to benefit unionizing physicians. As corporate entities using the PC-MSO and Friendly PC models seek to avoid adverse determinations as single or joint employers, physician unions may be able to gain concessions in bargaining in exchange for withholding a challenge on single or joint employment.
With physician unionization and corporate employment accelerating in recent years, these questions are no longer theoretical. For instance, a recent NLRB case considered a physician union challenge to the Friendly PC structure in California. There, the unionized physicians are directly employed by two professional corporations, Family Medicine and Healthcare Partners Medical Group. Those professional corporations are each solely owned by Dr. Derek Chao. Dr. Chao is the “friendly physician” installed by the professional corporation’s MSO, Optum, which is a subsidiary of the insurance conglomerate, UnitedHealth Group. Dr. Chao, in fact, works for Optum as the president of Optum West.
In the dispute before an NLRB regional director, the unionized physicians unsuccessfully argued that Optum should be considered a single employer.[8] The fact record demonstrated that Optum controls management and administration functions, employment of nonclinical staff, training, marketing, employment policies for physicians, and many other forms of control. However, the NLRB regional director found under a single-employer analysis that the entities did not comprise an “integrated enterprise.” The director here appeared to focus on the absence of a common owner of the distinct entities, finding that “the record is devoid of references to the specific entity known as Optum, Inc.” In a footnote, the director concluded that the union would also fail under a joint employer analysis, “based on the dearth of record evidence concerning that entity.”
The case has limited value given the undeveloped fact record and the sparse analysis of the joint employer question. But it is nonetheless relevant that the NLRB regional director found for Optum despite uncontroverted evidence of the Friendly PC model. That is, the fact that the sole owner of the formal employer (the medical practice) is a physician employed and paid by Optum was insufficient to conclude that Optum was a single employer. Future challenges, with more developed fact records, will help clarify how the NLRB interprets PC-MSO arrangements.
Joint employment questions are also bound to arise where physicians treating patients in a hospital setting are employed by corporate staffing companies. Today, one-third of emergency room physicians are employed by private-equity-backed staffing companies, such as Envision and TeamHealth. Hospitalists and other hospital-based physicians, such as anesthesiologists, are also increasingly employees of staffing companies. In California, a pending federal lawsuit is alleging that Envision’s use of the Friendly PC model violates the state’s CPOM ban. In Michigan, physicians at a hospital staffed by TeamHealth have unionized, and they recently went on strike. In all of these arrangements, the degree of control exercised by both the lay MSO and the non-employer hospital may supply grounds for single or joint employment status.
In a recent case of first impression, an NLRB regional director in Seattle found joint employer status to exist between a hospital system, PeaceHealth, and a staffing company, Sound Physicians.[9] The dispute involved a unit of thirty physicians, physician assistants, and nurse practitioners unionizing against Sound. The clinicians argued that while they were formally employed by Sound, the hospitals had direct influence on their terms of employment and were therefore joint employers. Sound argued that any control over terms and conditions of employment by the hospitals was indirect and merely a result of the contract between Sound and PeaceHealth for staffing support. The director, while expressly rejecting the 2023 heightened joint-employer standard, found Sound’s arguments to be unpersuasive. The director concluded that the hospitals exercised sufficient control over wages, benefits, hiring, discharge, and other employment-related issues to be a joint employer. Sound and PeaceHealth have appealed the decision.
Together, these recent cases suggest that more disputes over single and joint employment are forthcoming in the context of physician unionization. The regional decisions by the NLRB are not binding on other regions, though early decisions might have a persuasive effect. How physicians and employers strategically navigate these doctrines will be a development worth watching.
As corporatization of the medical profession continues, physicians are increasingly turning to labor law to collectively bargain over the terms and conditions of their employment. At the same time, state lawmakers and courts may be looking to strengthen CPOM bans that limit or prohibit direct employment of physicians, leading to the PC-MSO and other models of contractually complex employment relationships that will continue to evolve. Together, these factors raise the salience of the single and joint employer doctrines for physician unionization efforts, potentially allowing unionizing physicians to compel multiple corporate entities to comply with labor law rules set forth for employers. How courts and labor boards view these questions will influence the relative power of physicians in the context of unionization–and may influence rejuvenated efforts to enforce CPOM bans.
References
1] Zhu J, Rooke-Ley H, Fuse Brown E. A Doctrine in Name Only — Strengthening Prohibitions against the Corporate Practice of Medicine. N Engl J Med 2023;389:965-96.
[2] Rooke-Ley H, Fuse Brown E. Lesson’s From Oregon’s Attempt to Strengthen the ‘Corporate Practice of Medicine’ Ban. Health Affairs 10.1377/forefront.20240501.954346.
[3] NLRB v. Browning-Ferris Industries of Pennsylvania, Inc., 691 F.2d 1117, 1122 (3d. Cir. 1982).
[4] See Radio Union Local 1264 v. Broadcast Service, 380 U.S. 255, 256 (1965).
[5] Browning-Ferris Industries, 362 NLRB No. 186 (2015).
[6] James van Wagtendonk, Is There an Employer in the House?, 98 Boston L.R. 1105, 1107.
[7] U.S. Chamber of Commerce et al. v. NLRB et al., No. 6:23-cv-00553 (Mar. 8, 2024).
[8] Centers for Family Medicine, GP, and Healthcare Partners Medical Group, PC, Case 23-RC-311869 (2023).
[9] South Sound Inpatient Physicians, PLLC, and PeachHealth 19-RC-338479 (2024).
Wasan M Kumar, Stanford University School of Medicine
Contact: wkumar2@stanford.edu
What is the message? The May 2024 bankruptcy of Steward Health Care – the largest physician-owned hospital system in the country and one of the largest U.S. private hospital systems – raises questions about the hospital’s private equity funding, debt-financed business model and the future care of its patients.
What is the evidence? News reports, court documents, and company announcements.
Timeline: Submitted: June 3, 2024; accepted after review June 11, 2024.
Cite as: Wasan M Kumar. 2024. Steward Health Care: A Cautionary Tale. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 2.
In May 2024, Steward Health Care filed for bankruptcy with nearly $9 billion in liabilities, one of the largest hospital bankruptcies in US history.1 Steward’s financial collapse is closely tied to its private equity funding and debt-financed business model, leaving policymakers with questions about care delivery for the former Steward patients and scrutiny of private equity investment in healthcare.
Steward was launched in 2010 after a private equity firm, Cerberus Capital Management, acquired a failing nonprofit Massachusetts hospital system, Caritas Christi Health Care.2 Ralph de la Torre, a cardiac surgeon with degrees from Harvard Medical School and Massachusetts Institute of Technology, joined Caritas as CEO in 2008 after being recruited from Beth Israel Deaconess Medical Center, and remained as CEO for the new Steward Health Care.3 Steward was intended to show how an injection of private capital and the management model of private equity can be used to improve the management capacity and the services of a safety net healthcare system. At the time, de la Torre was quoted, “We are striving to further improve the quality of care our patients receive, attract talented new physicians, upgrade and expand the infrastructure at our facilities, maintain or grow our staffing levels and undertake additional investments to further improve the quality of care we provide. In Cerberus, we found an investor that shares our vision and commitment.” 2 This marked a substantial private investment in a large hospital system that predominantly delivered care to low-income patients on Medicaid or Medicare. The terms of the transaction were later modified, but finally approved, by the Massachusetts Attorney General.4
Steward grew from the six Caritas Christi hospitals in 2010 to 33 hospitals at bankruptcy in 2024.4
After failing to achieve profitable status or expand outside of Massachusetts, Steward sold its Massachusetts properties to Medical Properties Trust (MPT), a real estate investment trust (REIT), in a $1.25 billion sale-leaseback agreement in 2016.4 In a sale-leaseback agreement, organizations offload properties for a capital infusion, with an agreement to lease the facilities from the new property manager. Steward’s agreement included a 10-year escalator clause leading to annual rent increases, with each individual hospital responsible for rent, insurance, and taxes.
Steward used the funds it raised to make a payment to Cerberus capital, and then to acquire IASIS Healthcare in 2017 and expand to 36 hospitals across 10 states.3,5 In 2018, Steward became an international health system with operations in Malta and Columbia.
In 2020, de la Torre led a buyout of the remaining Cerebus interest in Steward, leaving ownership to a physician group (90%) and MPT (10%).5
As a result of the sale-leaseback agreement, the Steward system, which already failed to attain profitability by 2016, began experiencing increasing operating costs and worsening budgetary pressures given the large and increasing lease payments. Adding to the financial instability, Steward fell behind in its accounts payable to vendors who repossessed medical equipment needed for patient care. This was linked to adverse patient outcomes, including one patient’s death.6
The financial model for Steward remained challenging. In late 2023, Steward delayed lease payments to MPT, so MPT publicly announced efforts to recover its overdue payments and limit its exposure to Steward in January 2024.7 Negotiations to financially restructure Steward were unsuccessful, leading to the bankruptcy filing of Steward and 166 related entities in May 2024.8 In their filings, Steward reported $1.2 billion in secured debt and $8 billion in unsecured debt.8 Steward reported the full potential impact of this bankruptcy when they report that they served “two million patients annually, and employing a workforce of nearly 30,000. Since its inception, Steward has become a national, integrated health care network across 10 states comprised of 31 hospitals and over 400 facility locations (including physician practice offices, ambulatory surgical centres, and diagnostic imaging centres) with over 4,500 primary and specialty care physicians, all committed to serving patients in underinsured and underserved communities.”8
This was a stunning turn of events for Steward, leading to significant questions about the financial engineering underlying all of these transactions. Publicly, politicians were screaming about the two yachts and two jets owned by de la Torre.9 They demanded greater transparency and accountability for Steward’s management.10
Given the implications of the Steward collapse for patients and government-sponsored insurance, federal and state governments have grounds to scrutinize some of the financial tools used to construct Steward, including its REIT financing model. In 2021, REITs owned over $3.5 trillion in assets, with ownership of 3% of all hospitals nationwide.11 Medical institutions are particularly attractive for REITs, as these organizations are often willing to enter longer term sale-leaseback agreements that are negotiated for decades-long leases and have a predictable revenue stream.12 Healthcare organizations have stable cash flows, yet in this instance essential services were put at risk. From the perspective of investors, investing in these organizations can be risky, with Cereberus capital profiting approximately $800 million over 10 years,13 while MPT attributed $693 million in losses in Q1 2024 to Steward.14
The obvious question remains if sale-leaseback agreements even have a place in healthcare, and whether these institutions have the governance structure required to support these transactions. The short-term fiscal benefits of a sale-leaseback agreement could be very lucrative to hospital executives, but they may not support sustained growth of the underlying institutions. From the data currently available, its unclear if the REIT structure itself was at fault, or the escalation terms built into the REIT payments – presumably to help support operational cash-flow in the short term in exchange for higher payments in the future that might only occur by abandoning the safety-net patient base of the organization in the search for patients with more generous commercial insurance. Safeguards could be required in the terms of a sale-leaseback to prevent capital expenditures without an established plan for the hospital system to maintain its new fiscal responsibilities. In addition, the government could regulate sale-leaseback terms in healthcare to prevent hospitals from entering very long-term agreements or unfavorable escalator clauses. Of course, the Steward bankruptcy is also a cautionary tale for the REIT industry which supported an aggressive growth plan by Steward that ultimately failed.
The bankruptcy of Steward Health Care, the largest physician-owned hospital system in the country and one of the largest U.S. private hospital systems, could serve as a wake-up call for further examining the role of private equity in healthcare, especially in the hospital and safety-net markets. Of course, the investment industry will argue that Steward is a case of management greed and failure and should not serve as the condemnation of all of private equity. The inevitable investigations that will follow will shed further light on these questions.
In the immediate term, the crisis leaves lawmakers with several urgent questions to prevent the loss of care continuity for patients served by this hospital system. With Massachusetts often serving as a trailblazer in healthcare policy, the outcome of the Steward Health bankruptcy may set the tone for national health policy on private equity investment in healthcare.
References
We’re very excited to bring you this issue of HMPI. Thanks to a generous gift from the Ludy Family Foundation, we have been able to reformat HMPI for its second decade. The biggest changes are behind the web page where we have formatted the journal for Google Scholar with searchable meta-data. Many thanks to Managing Editor Kirsten Gallagher and her team for the hard work to make this transformation happen! Beyond the new format, you’ll see articles we have solicited on timely topics in the health care market.
One perspective missing from the drug re-importation debate in the US is that of Canada. In our featured article, we will learn Paul Grootendorst how the Canadian government and Canadian manufacturers have built legal mechanisms to protect their market and their drug supply. Medicare Advantage is in the news and is studied in many of our programs as a financial model, but what is it like to experience Medicare Advantage from the perspective of an enrollee. We have a very personal account of end-of-life care from Neil Fleming. PBMs constantly confuse students (and policy makers) on their role in the market. Rena Conti, one of the country’s experts on this industry, provides a careful overview of PBMs, some of their potential benefits and some of their challenges.
Reimbursement remains a challenge for many new medical products. New data document the barriers to establishing reimbursement codes from the innovators perspective. Prior authorization is also in the news. We’re grateful for a timely review of this health plan feature from Austin Allen and Markus Saba. Other articles this month include perspective on organizational innovation from Dick Levy, who built Varian and has served on over 20 public and private boards, an update on CMS price transparency rules from Steve Parente, who helped develop this policy during his time in the White House, a review of the University of Miami’s latest healthcare conference from Karoline Mortensen, Steven G. Ullmann, and Richard Westlund, and workforce challenge recommendations by the winners from our 2024 BAHM Case Competition, Angela Botiba, Divine Mercy Bakare, and Erika Schlosser. Finally, we have a new case study on administrative costs, and an overview of Robert Pearl’s new book.
Kevin Schulman, MD, MBA
BAHM President & HMPI Editor-in-Chief
Professor of Medicine, Stanford University
Neil S. Fleming, Robbins Institute of Health Policy & Leadership, Hankamer School of Business, Baylor University
Contact: Neil_Fleming@Baylor.edu
What is the message? Medicare Advantage plan enrollment now exceeds 50% of the total Medicare beneficiary population. MedPAC estimates that private insurers are now being paid at a higher level than the cost of enrollees within traditional Medicare, increasing total Medicare spending. This essay argues that pressure to reduce that spending is incentivizing Medicare Advantage plans and their contracted providers to favor financial considerations rather than the needs of terminally ill patients and their families.
What is the evidence? A first-person account around the decision to engage hospice care and the actions by providers in the context of a Medicare Advantage plan and a contracted medical group.
Timeline: Submitted: February 8, 2024; accepted after review April 16, 2024.
Cite as: Neil S. Fleming. 2024. Medicare Advantage and Hospice Care: My Family’s Difficult Story. Health Management, Policy and Innovation (www.HMPI.org), Volume 9, Issue 1.
My story is a family saga involving Medicare Advantage (MA) and the incentives it might create for providers who influence hospice care for terminally ill individuals. My family’s experience represents the struggles facing a growing number of families due to policy and system-level factors in the current U.S. healthcare environment.
The current number of Medicare Advantage members has risen to 51 percent of total Medicare beneficiaries, with the forecast to reach 60 percent by 2030 (Neuman et al., 2024). It has been argued that many factors support this trend of increasing membership in MA plans, stemming from factors such as better convenience, benefits, and financial protection for beneficiaries as well as aggressive marketing by insurance companies.1 From a policy perspective, there is concern that MA plans are actually increasing overall Medicare spending as private insurers increase covered MA beneficiaries and are paid at a much higher level (by Medicare) than the cost of equivalent traditional Medicare. This is according to the most recent Medicare Payment Advisory Commission (MedPAC) public meeting.1,2 Approximately half of Medicare decedents received hospice care).2 Increasing MA enrollment coupled with financial pressures and use of hospice, set an increasingly complex stage for terminally ill patients and their families.
Both of my parents were academics at Case Western Reserve University (CWRU.) Dad received his MD in his late 40s after receiving his PhD in his 20s. Mom received her PhD four years after Dad, delayed after caring for me for my first three years. Both had distinguished careers: Mom was the first female department chair at CWRU, and later finished her career at Cleveland State as Associate Dean of Education. They spent 20 wonderful years of retirement in Southern California after 34 years of often brutal winter weather in Cleveland, Ohio. My father’s increasing debilitation with Alzheimer’s forced my parents to move to Dallas to be closer to me, their only child, in mid-2012.
Dad only survived another nine months after their move. He mercifully suffered what was probably a stroke and passed with some of his cognitive abilities still intact (although he was still convinced he had traveled to the moon). My mother had undergone mitral valve repair surgery and a quadruple bypass in early 2008 back in California. By 2019, at 92, she experienced substantial valve leakage and suffered from advanced heart failure and failing kidneys.
When my parents first moved from California to Dallas, they were able to move into an independent living facility that was only 1.5 miles from my home. It was a comfortable existence, with a most convenient in-house primary care clinic offering access to both network specialty and hospital care coordinated as part of a Medicare Advantage plan. My parents left their traditional care coverage for this new option. Their increasing age and frailty, coupled with a local provider available by foot, made this an easy decision.
When Covid hit in early March 2020, only one caregiver was allowed access to the residents. I became that caregiver, which proved to be extremely important as Mom‘s heart ailments led to her continued decline. She began suffering from bouts of severe arrhythmia, which ultimately could not be ameliorated through ablation or medications. Finally, her electro-cardiologist admitted her into our local heart hospital for evaluation.
It took nine days of her inpatient stay for her medical team to sort out her electrical system, which resulted in the implant of a pacemaker. Looking back, that lengthy stay must have severely negatively impacted her individual risk spending metrics in relation to the premiums her Medicare Advantage program was receiving for her care. It would appear that her illness trajectory would present strong incentives to remove her from the MA plan by transitioning her into hospice care
Within the first week of my mother’s discharge, her primary care physician set up a post-discharge phone call with me. She announced in a clinical but assertive tone that my mother had at most six months to live and that we needed to begin planning for her transition to hospice care. Of course, this was terribly sad news and I shed many tears for what I later learned from our hospice grief counselor was “anticipatory grief.”
One night in June, as she continued to decline, my independent mother decided to forgo help from her night aide and fell on the way to the restroom. She suffered a broken wrist and, as can be expected, the cascading of events led to her final passing. Mom passed in July 2021, having lived 13 months rather than the less than the six months predicted by her physician.
As a side note, when my mother fell, her hospice nurse told us that all falls are considered related to the terminal condition. As a result, my mother had to sign an agreement that she would be financially responsible for all costs incurred related to the orthopedists’ services. I also worried about the prospect that she might need surgery and that we would be financially responsible for both professional and facility charges. However, the surgeon felt that her cast was sufficient for her arm to heal. This situation, which undoubtedly occurs often, appears to frequently burden people without necessary means and who may suffer from more debilitating injuries such as fractured hips or legs. This absolute cost shift to the patient felt cruel to us, like the system was “piling on” during one of the most stressful experiences a family, i.e., a dying parent and child, can endure. Mom’s hospice nurse was uncomfortable having this discussion with us, but we realized that she was simply the messenger.
My mother passed away with her cast still on.
To be clear, prior to the pacemaker implant expense, specialty care was never denied while Mom was still enrolled in her MA plan. Mom continued to receive expensive injections to slow her macular degeneration. We were also able to visit the local valve clinic to explore a transcatheter mitral valve replacement to address her leaky mitral valve problem. This option is much better for frail patients because it is much less invasive, although much more expensive. We decided that a new valve would be too risky for Mom, especially because it was addressing a repair (with subsequent biological challenges) rather than an initial valve repair or replacement. It was also unclear if it would substantially improve her quality of life amid the specter of unwanted complications. The Care Coordinator for her MA program was fantastic in seeking out care prescribed by all of Mom’s specialists during her entire membership.
I was a financial reviewer of health maintenance (HMO) risk arrangements in the1980s while serving as an external financial consultant for the Health and Human Services’ Office of Prepaid Health Care. I helped determine both federal qualification and compliance (the latter when HMOs ran into various financial and operational difficulties). I witnessed many types of contractual arrangements, some of which could put even the individual clinician as well as hospitals in the position of foregoing risk pool payouts. This aggressive form of risk sharing is not allowed under Medicare Advantage regulation.
Under 42 CFR § 422.208, “The MA organization makes no specific payment, directly or indirectly, to a physician or physician group as an inducement to reduce or limit medically necessary services furnished to any particular enrollee.”3
In retrospect, I queried long and hard: what would have caused Mom’s primary care physician to pronounce that she had less than six months to live? I was familiar with difficult “end of life” discussions, particularly as my former healthcare delivery system employer and clinicians were early champions of palliative care.6 I later learned that when terminally ill patients transition from Medicare advantage to hospice, the MA plan can no longer be at financial risk for medical services as the option for a move to traditional Medicare becomes available.2 As Mom was on the downward trajectory, the Medicare premiums received by her MA plan for services were clearly exceeded by her expenses for the care she had been receiving and most likely for future care. While this conclusion is clearly my educated speculation, Mom’s primary care physician and “gatekeeper” was accountable for her care and related costs, as well as indirectly responsible for the relationship between the medical group and the insurer of the MA plan. It now appeared to be in their “best interest” to preserve this relationship by jettisoning Mom and avoiding her medical costs as quickly as possible.
From a policy perspective, in the face of rising medical costs, there should be better ways to incentivize providers and insurers of MA plans to care for terminal patients, and especially those who are on hospice. However, one major positive from Mom’s physician’s pronouncement was that I spent as much time as possible taking care of her. I shared that responsibility with her caretaker during the day and with my wife and daughter during night and weekend duty. We had to employ care aides in the evenings and during the night, and we were fortunate to be in the financial position to afford them. While the unit cost of that care is not expensive, the number of units makes the total care expensive.
While remaining in the MA plan is apparently listed now as an option by CMS4, I do not recall that option being offered or explained. Rather, the hospice nurse told us that traditional Medicare would continue to cover non-terminal services per CMS. It seemed that the Medicare Advantage plan automatically transferred my mother from their plan to Medicare.
Medicare Advantage plans under the Affordable Care Act appear to have been created to produce greater certainty around federal outlays and budgeting by shifting risk, i.e., uncertainty, to external entities. Under global risk models, insurance companies have further shifted financial accountability to physician groups.5 Recent pushback has occurred as both physicians and hospitals have been declining contracts with insurance companies and their MA plans. Their rationale: increasing requirements to provide care have become burdensome for providers. They are no longer accepting their patients’ coverage, with patients bearing the brunt of these financial decisions. Patients are left to find new providers.7
The U.S. healthcare system remains complex and daunting, even for someone who has spent a 40-plus-year professional career studying and participating in the system. I have been employed by the federal government, a private insurer/administrator for a state Medicaid program, a consulting firm, a healthcare delivery system, and now, a university. Sadly, these broad experiences still do not prepare someone for the challenges of caring for a dying relative. The accomplishments and life experience both professionally and personally can matter little for the terminally ill and their families – although financial resources can alleviate at least some of worry. Medicare Advantage plans and their contracted providers will continually be incentivized to make decisions with increased weight on financial considerations rather than patient and family needs. One would hope, however, that the government and private payers could incentivize actions on the healthcare delivery side to be more humane during the struggles that families endure when a member is terminally ill.
References
Robert Pearl, Stanford University School of Medicine, Stanford Graduate School of Business
Contact: www.RobertPearlMD.com
ChatGPT, MD: How AI-Empowered Patients & Doctors Can Take Back Control of American Medicine, co-authored by Dr. Robert Pearl and the advanced AI system, ChatGPT, offers a unique perspective on the future of healthcare, highlighting the transformative potential of generative AI. All profits from the book go to Doctors Without Borders.
Dr. Pearl, a seasoned healthcare leader and author of Mistreated (a Washington Post bestseller) and Uncaring (a Kirkus star recipient), advocates for a future where AI and human collaboration redefine patient care and medical practice. The book begins with an exploration of medical history, “Generations,” tracing the evolution of healthcare from the groundbreaking diagnostics and therapies of the past century to the unfulfilled promises of more recent technological advancements. Dr. Pearl reflects on the transition from the pioneering era of Healthcare 1.0 (introduction of heart surgery, total joint replacement, transplantation, CT, MRI, etc.) to the two subsequent healthcare eras, characterized by electronic health records and telemedicine, which failed to live up to their potential due to systemic and cultural barriers. The narrative underscores a recurring theme: the loss of control by patients and doctors to corporate interests, leading to a healthcare system plagued by inefficiencies and declining clinical outcomes.
In part two, “Generativity,” the narrative shifts to medicine’s next phase, Healthcare 4.0, heralded by the integration of generative AI tools like ChatGPT into the healthcare ecosystem. Dr. Pearl points out the powerful economic forces at play in the United States, which will force American medicine to change, whether led from inside or outside of the current healthcare system. He elucidates the exponential growth trajectory of generative AI, predicting breakthroughs in personalized medicine, diagnostics, and therapeutics. He emphasizes that the successful integration of AI in healthcare hinges on overcoming existing systemic barriers and fostering a connected, collaborative, and patient-centric medical system.
“Genesis” delves deeper into the foundational changes necessary for the effective adoption of AI in healthcare. Dr. Pearl champions the concept of systemness, advocating for a unified approach that enhances patient care and addresses the burnout epidemic among clinicians. He highlights the potential of external disruptors like Amazon, CVS, and Walmart to catalyze innovation and underscores the need for clinicians to break from outdated norms to embrace the new paradigms enabled by AI.
In “Gently,” Dr. Pearl discusses the role of AI in alleviating clinician burnout by providing patients with medical expertise, allowing them to better manage their chronic diseases and enabling more fulfilling doctor-patient interactions. Dr. Pearl tackles the ethical considerations (privacy, security, bias, misinformation) and potential pitfalls of AI deployment in healthcare. He addresses common fears and skepticism towards new technologies, arguing that, as with past innovations, habituation will ease these apprehensions. The book advocates for regulatory frameworks that encourage, rather than stifle, AI innovation, ensuring that patient welfare remains paramount.
The concluding fifth part, “Next Gen,” highlights the crucial role of visionary leadership in realizing the potential of generative AI in healthcare. Through case studies and the practical “A to G” model, Dr. Pearl illustrates how effective leadership can guide healthcare professionals through the change process, overcoming skepticism and resistance. The final chapter, “Seizing Serendipity,” encapsulates the notion that medical miracles often result from the convergence of opportunity and preparedness. Here, Pearl and his co-author urges leaders to embrace the transformative possibilities of generative AI.
Blending Dr. Pearl’s insights with ChatGPT’s capabilities, this book offers actionable solutions for healthcare, providing a pathway for doctors and patients to take back control of medical practice from corporate entities and a compelling case for a future where technology and humanity converge to create a more efficient, personalized, and accessible healthcare system.