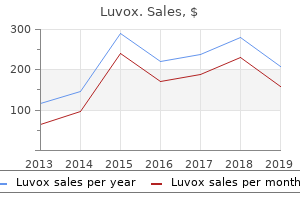
"Discount luvox 100mg with amex, anxiety treatment for children".
By: W. Finley, M.A., Ph.D.
Medical Instructor, Pennsylvania State University College of Medicine
Particularly important for phonation is the correct positioning of the muscles and cartilages of the larynx anxiety young living generic luvox 100 mg with amex, or voicebox anxiety symptoms in 9 year old boy discount luvox 50 mg with amex. The amount and speed of airflow also contributes to the type and quality of phonation anxiety symptoms lasting a week buy generic luvox pills, and to whether phonation will occur at all anxiety disorder symptoms yahoo purchase luvox 100mg otc. The larynx houses and protects the two small fleshy folds known as the vocal folds, or "vocal cords," which vibrate to produce the phonation that enables us to speak, and which give the larynx its common name, the "voicebox. The main cartilages of the larynx are the cricoid, the thyroid, the two arytenoids, and the epiglottis (see Figures 5. The trachea, briefly mentioned in Chapter 4, is a tube of horseshoeshaped cartilages with openings at the back. Interconnecting ligaments and mucous membranes between the cartilages make the trachea airtight. The thin back wall of the trachea is attached to the esophagus behind, and the tubes run parallel until the trachea diverts to the lungs and the esophagus diverts to the stomach. Attached to the top of the trachea is the base of the larynx the cricoid (Greek, "ring-like") cartilage, which is shaped like a signet ring, with the larger, flat part of the ring facing back toward the spine. On top of the cricoid cartilage sits the thyroid (Greek, "shield-like") cartilage, the largest of the laryngeal cartilages. It is composed of right and left plates that fuse at the front to form the shield-like structure from which the thyroid cartilage gets its name. The two plates fuse together to form a triangular-shaped notch, or angle, that can be felt from the outside. At the back of the thyroid cartilage are two superior horns and two inferior horns. The inferior horns rest on the surface of the cricoid cartilage so that the two cartilages can rock back and forth relative to one another, while the superior horns connect the larynx upward to the hyoid, a small bone in the root of the tongue (see Chapter 6). Just below the thyroid angle, the anterior ends of the vocal ligaments (the innermost part of the vocal folds) connect to the inside of the thyroid angle. The posterior ends of the vocal ligaments connect to the two arytenoid (Greek, "ladle-like") cartilages that rest on the thick part of the cricoid cartilage at the back of the larynx. The two tiny arytenoid cartilages are roughly pyramid-shaped, but hollowed out on one side like a ladle. The fronts of the arytenoids end in small protrusions called the vocal processes, which are the rear attachment points for the vocal folds. The muscular processes stick out behind and laterally, providing attachments for some of the intrinsic muscles of the larynx. The arytenoid cartilages have two primary movements: they can pivot on the cricoid cartilage or slide along its edge. Two miniscule bits of cartilage, the cuneiform (Latin, "wedge-shaped") and Hyoid Bone Epiglottis Corniculate c. The epiglottis is a flap of cartilage attached behind the angle of the thyroid near the root of the tongue, and projecting upward behind the tongue. During swallowing, the larynx is raised, and the epiglottis folds over to keep food from going down the trachea. Now that you know the names of the hard structures of the larynx, it will be easy to learn the names of the muscles that connect them. The vocal folds, despite their small size, are actually very complex (see Figure 5. From Flow to Sound 75 Hyoid Bone Glottis False Vocal Folds Vocal Folds Cricoid Cartilage Thyroid Cartilage Figure 5. The false vocal folds contain no muscles, and hence are not under direct muscular control, but in some speakers they can vibrate along with the true vocal folds, intentionally or unintentionally, which may result in a rough-sounding voice. Generally, however, the function of the ventricular folds in speech is not well understood. When these muscles contract, they pivot the arytenoid cartilages so that the vocal processes turn inward, adducting, or moving the vocal folds together (see Figure 5. Posterior Cricoarytenoid Transverse Interarytenoid Epilaryngeal Tube Aryepiglottic Fold Oblique Interarytenoid Lateral Cricoarytenoid Thyroarytenoid Posterior Cricoarytenoid Transverse Interarytenoid Figure 5. Transverse Interarytenoid Thyroarytenoid Oblique Interarytenoid Posterior Cricoarytenoid Lateral Cricoarytenoid Cricothyroid Figure 5.
We collected 2 anxiety symptoms back pain purchase online luvox,549 ticks from the field: 2 anxiety symptoms on kids order luvox 100 mg online,192 Amblyomma americanum (1 larva anxiety xiphoid process order luvox 50 mg online, 1 anxiety symptoms in children checklist buy discount luvox 50 mg on line,917 nymphs, 274 adults), 306 I. Post hoc comparisons indicated that tick density at the highest elevation site (9. Infection prevalence varied significantly among sites (likelihood ratio test, G = 16. Cases per 100,000 population were calculated by county or city census estimate data published for the year preceding the year of the report. Maximum-likelihood phylogenetic reconstruction using Tamura 3-parameter model (34) indicated that all haplotypes detected fall within the American clade; none of the ticks we sampled were phylogenetically identified as southern clade I. Taken together, these results suggest recent spatial and/or demographic expansion of I. VariationinestimatedprevalenceofBorrelia burgdorferi infection in Ixodes scapularis nymphs at 4 field sites in Virginia. Our data suggest that this vector species may be more abundant than it was before 2007; during widespread collections during 20042007, I. For example, on the basis of extensive sampling in the eastern United States over several years, Diuk-Wasser et al. An elevational threshold that limits tick populations at northern latitudes, where high elevation sites experience extreme cold during winter months, would not be expected where equivalent elevations are associated with more moderate climatic conditions. This discrepancy suggests a southwestward spatial expansion of northern tick populations into the upper Piedmont and mountain regions of Virginia or demographic expansion of persons into areas of previously low tick density in western localities. Moreover, analyses of single-nucleotide polymorphism data are consistent with south-to-north postglaciation gene Figure 4. However, we cannot exclude the possibility that the distribution of endemic American-clade ticks simply has expanded in Virginia. Southern-clade nymphs may have questing behavior that makes them unlikely to be collected on cloth drags or to bite humans (9); thus, nymphal ticks are difficult to collect, even in places where adult ticks are common. However, data from a single mitochondrial gene, albeit one that has been widely characterized for this species, do not necessarily reflect patterns of differentiation found in nuclear markers (21) and probably are not useful for delineating among behavioral phenotypes. Moreover, we sampled in daytime hours during the presumed peak period of nymphal activity (late spring, early summer) and thus would not have detected ticks exhibiting different host-seeking behaviors. It is possible that multilocus genomic analysis or year-round sampling would yield different insights from those reached in this study. Thesizeofeachcircle represents the annual number of cases reported by the Virginia Department of Health and is proportional to annual incidence (cases/100,000 population). Black arrow represents the mean linear direction of annual movement among centroids during 2006 2011 (these years indicate the recent dramatic increase in Lyme diseaseincidenceinVirginia). As a result, clinicians and epidemiologists need to be vigilant in the face of changing spatial distributions of risk, especially in transition zones where patterns of disease are rapidly changing (40). Spicer for assistance with sample collection and processing of laboratory samples. We also thank 2 anonymous reviewers for their thoughtful comments on an earlier draft of this manuscript. Dr Brinkerhoff is an assistant professor at the University of Richmond and holds an honorary senior lectureship in the School of Life Sciences, University of KwaZulu-Natal, Pieter maritzburg, South Africa. His research focuses on the ecology, evolution, and epidemiology of bacterial pathogens transmitted by arthropod vectors. Ecological studies of adult Ixodes scapularis in central Mississippi: questing activity in relation to time of year, vegetation type, and meteorologic conditions. Maurelli Shiga toxins (Stx) are cytotoxins involved in severe human intestinal disease. These toxins are commonly found in Shigella dysenteriae serotype 1 and Shiga-toxinproducing Escherichia coli; however, the toxin genes have been found in other Shigellaspecies. Weidentified26Shigella flexneri serotype 2 strains isolated by public health laboratories in the United States during 20012013, which encode the Shiga toxin 1a gene (stx1a). These strains produced and released Stx1a as measured by cytotoxicity and neutralization assays using anti-Stx/Stx1a antiserum. The release of Stx1a into culture supernatants increased 100-fold after treatment with mitomycin C, suggesting that stx1a is carried by a bacteriophage. Infectious phage were found in culture supernatants and increased 1,000-fold with mitomycin C. Furthermore, all patients who reported foreign travelhadrecentlybeentoHispaсiola,suggestingthatemergence of these novel strains is associated with that region.
The general dentist must also confirm with the specialist any need for future treatment or reevaluation anxiety symptoms reddit buy generic luvox 50mg line. A classic example is the orchestration of periodontal maintenance treatment between the periodontist and the general dentist anxiety meditation discount luvox. Other examples include periodic evaluation of implant therapy and treatment for pathologic oral conditions anxiety symptoms returning order luvox 100 mg without a prescription. Periodontal Therapy In a dental school environment anxiety upper back pain buy luvox 50 mg online, initial periodontal therapy often is sequenced first in a treatment plan. Although this may be appropriate for the individual with few additional treatment needs, it may not be appropriate for others, especially those who are having some discomfort. To ensure appropriate care, periodontal therapy should occur as early as possible in the plan, but it can be delayed for several reasons. One frequently encountered justification is the decision to first resolve a simple complaint, such as replacing a lost restoration or extracting symptomatic impacted third molars. Another example is the patient with large carious lesions, especially those located subgingivally. Restoring such teeth with a permanent or provisional filling should make periodontal treatment more comfortable for the patient, and begin to resolve the gingivitis that accompanies subgingival lesions. Lastly, teeth that are nonrestorable or are periodontally hopeless are often extracted before beginning scaling and root planing procedures. This typically occurs when the patient has not seen a dentist for many years, and the dentition is covered with plaque and calculus. The dentist may decide to begin gross scaling of the teeth to permit visualization and exploration of tooth surfaces during the examination. Caries Control For the patient with many carious lesions, treatment consists of restoring lost or decayed tooth structure and preventing caries from occurring in the future. The following guidelines should be followed when triaging treatment for caries: · Address any symptomatic teeth first. Extract those that should not be retained for obvious periodontal Chapter 3 Developing the Treatment Plan 65 or restorative reasons. For other symptomatic teeth, remove all caries, begin endodontic therapy if necessary, and place a permanent or provisional restoration. The goal is to prevent symptoms for the patient and avoid irreversible injury to the pulp. For teeth with caries at or below the alveolar crest radiographically, remove the caries and decide whether the tooth can be restored (Figure 3-4). Endodontic therapy should not be provided until the tooth is deemed restorable and periodontally sound. Endodontic Therapy Endodontic therapy consists of a series of treatments, including removing pulpal tissue, filing and shaping root canals, obturation of the root canal space, and placement of a permanent restoration for the tooth. For some patients, it may be appropriate to do each step in succession, especially when no other problems have been identified. For patients with many deep carious lesions or pulpal pain, simply removing the caries and pulpal tissue followed by rudimentary filing and shaping and placement of a provisional, sedative restoration is preferred. After establishing some level of disease control, endodontic therapy can then be completed. To prevent fracture, permanent restorations for endodontically treated teeth should be sequenced before those for vital teeth if at all possible. Extraction When possible, tooth extractions should be sequenced early in the treatment plan to permit healing to take place, especially before tooth replacements are fabricated. The dentist should attempt to limit the number of surgical appointments and extract all hopeless or nonrestorable teeth at the same time. It may be necessary to delay the extraction of asymptomatic teeth so that provisional replacements can be fabricated to preserve appearance, to maintain the position of opposing and adjacent teeth for short periods of time. The classic example of this concept involves planning to place immediate dentures. The process begins by removing the posterior teeth, leaving the anterior teeth for esthetic reasons. Impressions for the dentures are taken 6 to 8 weeks later, after some healing of the posterior segments has occurred.
Before a pulp cap is placed anxiety 18 year old buy luvox overnight delivery, all treatment options and the possible consequences of each must be described to the patient i have anxiety symptoms 247 luvox 50mg free shipping, including the fact that a significant percentage of direct pulp caps can be expected to fail anxiety symptoms postpartum order luvox now. Initially the direct pulp cap should be considered as an interim solution by both patient and practitioner anxiety symptoms upper back pain purchase luvox 50 mg without a prescription. If, on reevaluation, the tooth remains asymptomatic, with vital pulp tests and no evidence of apical pathology either clinically or radiographically, then the expectation of long-term service can be given qualified endorsement. A direct pulp cap can be considered an interim treatment when there has been a direct exposure of the pulp and pulpal necrosis is imminent-but the patient either wishes to have the tooth extracted at a future date or cannot decide whether to try to save the tooth or to extract. For either alternative, a clear time interval must be established, at the conclusion of which the patient must make a decision. In this situation, it is essential that the patient be informed that there is strong likelihood of further problems, especially pain or infection if the tooth is left unattended. Irreversible Pulpitis or Necrotic Pulp In this situation, definitive pulpal therapy with root canal treatment or extraction is required. Only if the practitioner is unable to execute a complete pulpectomy or tooth removal at the same visit should a partial pulpectomy or pulpotomy be considered, and the patient must understand that this is not a definitive form of treatment. Patient Declines Treatment for an Asymptomatic Apical Periodontitis, Cyst, or Granuloma When definitive pulp therapy is indicated and the patient, for whatever reason, declines treatment, the clinician is presented with a dilemma. If the patient suffers from an immunocompromising condition, allowing chronic apical infection to persist would, in most cases, be inappropriate and unacceptable. For the patient with a normal host response, the dentist may elect to reevaluate the condition at specified periods as discussed in Chapter 9. Some clinicians never allow chronic apical lesions to go untreated and certainly this approach has Chapter 7 the Disease Control Phase of Treatment 163 merit. Even in cases in which root canal therapy might otherwise be deferred, common sense dictates that when a restoration is planned for the tooth, the root canal treatment should be performed first. Single Tooth Restoration in the Disease Control Phase of Care A tooth that is to be restored as part of the disease control phase, but for which root canal therapy is not necessary or warranted, normally receives a direct-fill definitive restoration as discussed in Chapter 8. If the tooth is found to require a crown in the definitive phase of care, a core or foundation is placed during the disease control phase using a direct-fill restorative material. This treatment serves as both an interim restoration and the base upon which the definitive restoration is to be placed. In rare cases, usually associated with a compelling esthetic concern for which a composite restoration will not suffice or when there is no other satisfactory way to provisionally restore the tooth, an indirect partial or full coverage restoration is warranted during the disease control phase. Once the root canal treatment is complete, a more long-term provisional or definitive restoration is necessary. When an anterior tooth has had root canal treatment, but insufficient tooth structure remains to support a composite restoration, a provisional post and crown is typically constructed. Another interim solution is to fabricate the definitive post and core and follow up with a provisional or definitive full coverage restoration. In any case, it is absolutely necessary to maintain an effective seal between the oral cavity and the root canal filling material. Stabilization of Dental Malalignment, Malocclusion, or Occlusal Disharmony Most problems related to the malposition or malocclusion of teeth are addressed in the definitive phase of the treatment plan and are discussed in Chapter 8. It is usually inadvisable to seriously consider orthodontic treatment before disease control therapy has been successfully completed. In some instances, however, occlusal or limited orthodontic therapy can or should be accomplished as part of a comprehensive disease control program. Root Proximity Problem That Precludes Restoration of a Carious Lesion or Fracture In the presence of a large proximal carious lesion, adjacent teeth may drift together (Figure 7-15). To gain access for caries removal and to place a matrix band and restoration with a physiologic contour, it may be necessary to orthodontically separate the teeth. Plunger Cusp, Open Contact, and/or Marginal Ridge Discrepancy Contributing to Food Impaction and Periodontal Disease Presence of a plunger cusp may encourage food impaction, and the soft tissue in the area may be red, bulbous, and swollen, with tender papillae and bleeding on probing. In this situation, a judicious recontouring of the offending cusp may be in order.
Order discount luvox online. The Effect of Access Bars on Anxiety & Depression - with Dr. Dain Heer & Dr. Terrie Hope.