"100 mg viagra soft, impotence juice recipe".
By: B. Ressel, MD
Medical Instructor, Florida International University Herbert Wertheim College of Medicine
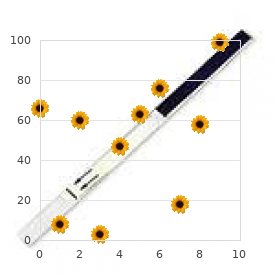
These properties render citrate the most effective chelator of calcium in the urine erectile dysfunction shake cure cheap 100 mg viagra soft visa, which prevents its precipitation with phosphate and oxalate (48 zinc causes erectile dysfunction buy viagra soft 50 mg mastercard,49) erectile dysfunction 43 purchase 50 mg viagra soft overnight delivery. Hypocitraturia is a major underlying cause of human kidney stones and erectile dysfunction treatment washington dc purchase viagra soft with a mastercard, thus, citrate is the most important urinary anion for clinicians to understand (49). Phosphate Transport Phosphate homeostasis at the whole-organism level involves coordinated fluxes in the intestine, bone, and kidney, and endocrine cross-talk constituting a complex multiorgan network (50). Although both the intestine and bone are critical organs for phosphate homeostasis, this manuscript will only discuss the renal component. It is important to state that intestinal phosphate absorption involves significant paracellular uptake that is poorly regulated (51). Unlike Na1 reabsorption where the finishing fine-tunings are achieved by more distal segments, phosphate reabsorption is accomplished almost entirely by the proximal tubule (52). A small contribution from the distal tubule has been proposed, but is still disputed (53). Plasma levels reflect total body phosphate status but are very insensitive; spot urinary concentrations are confounded by water excretion rate; and excretion rates of phosphate are affected by ingestion. Thus, all of these parameters are less than ideal to evaluate renal tubular phosphate handling. The parameters listed in Figure 4A are better suited to probe the proximal tubular handling independent of the excreted or filtered load. The flux of filtered and reabsorbed Pi is plotted against plasma phosphate concentration; the difference between the two yields the rate of excretion of Pi. The maximal tubular reabsorptive capacity of Pi (TmP in units of mass/time) refers to the saturating transepithelial flux of Pi that the tubule can mount and is equal to the difference between filtered and absorbed phosphate when the filtered load is higher than TmP. Three apical transporters mediate Pi entry with different preferred valence of Pi, stoichiometry of Na1, electrogenicity, and pH gating. The affinities for Na1 are all approximately 3050 mM but are much higher for phosphate (0. Apical Na-coupled Pi transport is inhibited in acidosis by alteration in luminal substrate, directly gating of the transporter by pH, and decreased apical NaPi transporters as described in Figure 3B. The disparate properties of the three transporters were reviewed in great detail by Virkki and colleagues (54). It is possible that one or more of the plethora of anion exchange mechanisms may mediate phosphate exit. Regulation of phosphate transport at the proximal tubule apical membrane is precise because this is the only and final site of determination of extracellular phosphate balance by the kidney. Phosphate uptake is affected by incoming signals, such as parathyroid hormone (55), dopamine (56), fibroblast growth factor-23 (57), and Klotho (58), which inhibit phosphate transport and induce phosphaturia. One of the most potent regulators of phosphaturia is dietary phosphate intake itself, which may involve a variety of hormones, including unknown intestinal enterokines (59), and direct sensing by the proximal tubule (60). This is one of the most important, yet least known, areas in phosphate homeostasis. The modulation of proximal phosphate transport is achieved largely by trafficking of the transporters in and out of the apical membrane (52) with the exception of Klotho, which can directly affect phosphate transport activity (58). Response to Acidosis the catabolism of acidic and sulfur-containing amino acids results in the net production of acids. As a result, a high-protein diet leads to a mild chronic metabolic acidosis that is usually well compensated. The common clinical condition of metabolic acidosis is characterized by a more significant decrease in plasma pH and bicarbonate concentration. This disturbance in acid-base balance can be caused by genetic or acquired alterations in metabolism, in renal handling of bicarbonate, and in the excretion of acid. Chronic acidosis also causes impaired growth, bone loss, muscle wasting, nephrocalcinosis, and urolithiasis. An essential renal compensatory response to metabolic acidosis is initiated by increased extraction and catabolism of plasma glutamine that occur predominately in the proximal convoluted tubule. The resulting increases in renal ammoniagenesis and transport into the urine accomplish the excretion of acid, whereas the increased bicarbonate synthesis and transport into the blood partially correct the systemic acidosis. These adaptations occur rapidly after acute onset of acidosis and are subsequently sustained by more gradual changes in gene expression. During normal acid-base balance, the kidneys extract and metabolize very little of the plasma glutamine. Although approximately 20% of the plasma glutamine is filtered, the measured rat renal arterial-venous difference is,3% of the arterial concentration of glutamine (61), and only 7% of the plasma glutamine is extracted by the human kidneys even after an overnight fast (62).
Propofol erectile dysfunction caused by anabolic steroids order viagra soft 50 mg free shipping, a short acting anaesthetic agent erectile dysfunction causes mnemonic purchase discount viagra soft on line, reduces intracranial pressure but causes systemic vasodilatation erectile dysfunction latest medicine viagra soft 50 mg low cost. If this occurs pressor agents may be required to prevent a fall in blood pressure and a reduction in cerebral perfusion erectile dysfunction venous leak generic 50 mg viagra soft free shipping. Avoid high doses of Propofol; rhabdomyolysis may result and carries a 70% mortality. Barbiturates (thiopentone) reduce neuronal activity and depress cerebral metabolism; a fall in energy requirements theoretically protects ischaemic areas. Associated vasoconstriction can reduce cerebral blood volume and intracranial pressure but systemic hypotension and myocardial depression also occur. Clinical trials of barbiturate therapy have not demonstrated any improvement in outcome. Although this reduces intracranial pressure, the resultant reduction in cerebral blood flow may aggravate ischaemic brain damage and do more harm than good (see page 232). The principal concern is that although reducing mortality, unacceptable levels of morbidity may result. A randomised trial of decompressive craniectomy in head injury is currently underway. Although hypothermia after cardiac arrest with slow rewarming has been reported to improve outcome, trials in head injured patients have failed to demonstrate significant benefit. Steroids: By stabilising cell membranes, steroids play an important role in treating patients with oedema surrounding intracranial tumours. Many pathological processes may impair conscious level and numerous terms have been employed to describe the various clinical states which result, including obtundation, stupor, semicoma and deep-coma. These terms result in ambiguity and inconsistency when used by different observers. Recording conscious level with the Glasgow coma scale (page 5) avoids these difficulties and clearly describes the level of arousal. Lesions diffusely affecting the cerebral hemispheres, or directly affecting the reticular activating system cause impairment of conscious level: Diffuse hemisphere damage. Prognosis Although conscious level examination does not aid diagnosis, it plays an essential role in patient management and along with the duration of coma, pupil response and eye movements provides valuable prognostic information. This results from: Syncope: Reduction in cerebral arterial oxygen supply can be caused by cardiac arrhythmias, cardiac outflow obstruction or vasovagal attack. Seizure: Pseudo-seizure (non-epileptic attack disorder) see below Acute toxic or metabolic coma: Drug abuse alcohol, solvents or barbiturates may cause transient, intermittent confusion. History from the patient: Context: may suggest likely cause a collapse when having blood taken suggests syncope; an episode arising from sleep suggests a seizure. Prodrome: a brief sensation of dйjа vu before the episode indicates a focal onset seizure; a feeling of lightheadness, sweatiness and visual fading suggests syncope. Recovery: a rapid recovery suggest syncope; waking in the ambulance suggest seizure. History from witness (find them; phone them): How long the patient was out for; syncope is typically less than 1 minute; seizures usually longer. What they did; brief asynchronous jerking movements occur in syncope; more prolonged synchronous tonic clonic movements occur in seizures. Silent witnesses: Incontinence is common in all forms of loss of consciousness and does not distinguish between a seizure and syncope. Tongue biting strongly suggests a seizure as do other much less common injuries posterior dislocation of the shoulder or vertebral fracture. Head up tilt-table testing may reveal neurocardiogenic syncope or orthostatic hypotension. Often attacks of unconsciousness remain unexplained and possibly have a psychological basis. Such attacks are often mistaken for a seizure and are referred to as pseudo-seizures or non-epileptic attacks (see page 99). Most patients are easily distracted, have slowed thought processes and a limited concentration span.
Mechanical forces are important regulators of the activity of renal ion channels (1825) erectile dysfunction stress treatment viagra soft 50 mg fast delivery, as well as of the signaling activities that regulate renal ion and fluid transport (14 erectile dysfunction karachi order line viagra soft,2628) erectile dysfunction over 50 buy discount viagra soft 100mg. Therefore erectile dysfunction interesting facts buy cheap viagra soft on line, the capacity to monitor mechanical sensations is exploited by the kidney in its efforts to maintain homeostasis. In this review, we discuss recent studies that reveal surprising and important roles for mechanosensitive and chemosensory molecular machinery in renal function. These cilia arise from the apical surfaces of the epithelial cells and protrude into the tubule lumen. Just beneath the ciliary membrane is the ciliary axoneme, which is a scaffolding composed of nine doublet microtubules that are parallel to one another and that extend from the base of the cilium along its entire axial length. In contrast with the motile cilia that are found on airway and oviduct epithelial cells, primary cilia, such as those found on renal epithelial cells, do not beat and do not move fluid. Instead, their function appears to be entirely sensory and their structure reflects their sedentary nature. The axonemes of motile cilia possess a central pair of microtubules that is connected by radial spokes to the nine doublet microtubules at the ciliary periphery. These additional components include the motor proteins that allow motile cilia to generate force. Although primary cilia, such as those found in the kidney, lack these components found in their motile cousins, they are by no means devoid of motor proteins. It should also be noted that every cilium arises from a basal body, which is a structure composed of paired cylindrical assemblies of microtubules. The basal body serves as the centriole that organizes the mitotic spindle in dividing cells. A complex array of proteins connects the base of the axoneme to the basal body and forms the ciliary transition zone, which serves as a barrier that helps to maintain the compositional distinctions between the apical and ciliary membrane domains (34,35). Although the structure of the renal primary cilium is fairly well understood, the same cannot be said of its function. It is clear that the cilia of renal epithelial cells serve extremely important purposes, as evidenced by the large number of renal phenotypes arising from mutations in genes whose products participate in ciliogenesis (36). These pleomorphic conditions are characterized by partially overlapping lists of neurologic, skeletal, metabolic, and sensory phenotypes, including renal cystic disease. In addition, the proteins encoded by the genes responsible for both the autosomal dominant and autosomal recessive forms of polycystic kidney disease localize, at least in part, to the primary cilium (3941). On the basis of this brief summary, it might be logical to suggest that the cilium participates in sending signals that are required to prevent the development of renal cysts. The groundbreaking work of Praetorius and Spring revealed that the primary cilium can detect and respond to mechanical stimuli (42). These investigators showed that either direct or flow-induced bending of the primary cilia of cultured renal epithelial cells led to the activation of ion channels that mediated calcium influx, which secondarily activated calcium release from intracellular stores. Studies into the function of the proteins encoded by the autosomal dominant polycystic kidney disease genes (41) have provided insight into the nature of the mechanosensitive ion channels responsible for this cilia-dependent activity. Polycystin-2, encoded by the Pkd2 gene, is roughly one fourth of the size of polycystin-1 and spans the membrane 6 times. Polycystin-1 and polycystin-2 interact with one another to form a complex that localizes in part to the cilium and that may contribute to the calcium channel activity that is induced by ciliary bending. This activity may depend upon TrpV4, another membrane of the Trp family of cation channels whose channel activity may be regulated in some manner by the polycystin proteins (43). These observations have inspired a model in which the ciliary population of the polycystin-1 and polycystin-2 complex serves as a sensor that transduces tubular fluid flow to produce an elevation of renal epithelial cell cytoplasmic calcium concentrations (44). These observations prompt the further suggestion that loss of this mechanically activated polycystin channel activity, or of the mechanosensitive cilium in which this activity resides, could lead to the perturbations in cell proliferation, differentiation, and fluid secretion that together characterize the formation of autosomal dominant polycystic kidney disease renal cysts. Recent data indicate that close relatives of polycystins, rather than the polycystin-1 and polycystin-2, may mediate ciliary ion currents in at least some cell types (45,46). Although the role of the ciliary polycystins as flow sensors is intriguing, it seems quite likely that these proteins also participate in other sensory processes. In addition to their connection to cytoplasmic calcium levels, the polycystin proteins have been connected to a very large and diverse collection of signaling pathways that have the potential to influence cellular growth and metabolism (41). Finally, it is worth noting that both polycystin proteins have homologs that have been shown to serve as chemosensors. Polycystin-1like-3 and polycystin2like-1 form a complex that detects low pH, serving both as sour taste receptors in the tongue and as sensors of pH in the central nervous system (1,48,49). Taken together, these facts suggest that the polycystins may serve chemosensory roles in renal epithelial cells.
Patients may also complain of weakness with motions that involve abduction and external rotation erectile dysfunction doctors in cincinnati order viagra soft 50mg with mastercard, especially in those patients with suprascapular nerve entrapment proximal to the supraspinatus muscle erectile dysfunction zinc supplements purchase 100 mg viagra soft with amex. Although a distinct traumatic injury is identified in nearly half of patients with suprascapular neuropathy [111] erectile dysfunction doctor omaha order viagra soft 100 mg fast delivery, most cases are the result of chronic traction from repeated overhead activity such as those who participate in overhead sports and heavy manual labor how to fix erectile dysfunction causes cheap viagra soft 100 mg on-line. As mentioned above, suprascapular nerve injury should also be suspected in patients with massive, retracted supraspinatus tears [91, 92, 112] in addition to those who have undergone previous shoulder surgery. Perhaps the most important physical examination findings in patients with suprascapular neuropathy are those obtained via simple inspection of the affected shoulder. The presence of surgical scars over the posterior shoulder should raise concern for nerve entrapment as a result of scar tissue and adhesions. The most common procedures resulting in nerve entrapment include rotator cuff repair, posterior approaches to the glenohumeral joint and, in one case, distal clavicle excision [113]. Prominence of the scapular spine may indicate atrophy of both the supraspinatus and infraspinatus muscle bellies, especially in cases of suprascapular nerve entrapment at the suprascapular notch. When nerve entrapment occurs more distally at the spinoglenoid notch, isolated atrophy of the infraspinatus muscle belly can be appreciated. If periscapular muscle wasting occurs simultaneously with rota- tor cuff muscle atrophy, a more proximal lesion should be suspected, such as the C5 nerve root from which the dorsal scapular nerve arises, thus highlighting the importance of a complete neurovascular examination. The supraspinous fossa, infraspinous fossa, and acromioclavicular joint may be tender to palpation in those with nerve entrapment at the suprascapular notch. In contrast, the patient with nerve entrapment at the spinoglenoid notch may be tender to palpation near the posterior joint line. Active and passive range of motion should be tested in all patients to determine the degree of clinical weakness and the potential effects of general shoulder stiffness and scapular dyskinesis on the chief complaint. There are no specific provocative maneuvers designed specifically for the detection of suprascapular neuropathy; however, it is postulated that humeral adduction and internal rotation may be useful to reproduce symptoms in patients with tension-type suprascapular nerve injuries since a study by Plancher et al. When suspected, other provocative maneuvers may be necessary to detect concomitant pathologies such as labral tears, rotator cuff disease, glenohumeral instability, and/or scapular dyskinesis. The nerve is tethered to the middle scalene and the neural pedicle of the serratus anterior which explains its high rate of traction-type injuries. The patient is asked to perform a push-up against a nearby wall as if the patient were in the prone position. Note the prominence of the medial scapular border which is a characteristic feature of long thoracic nerve palsy. Typically, the injury occurs when the arm is elevated overhead with the neck rotated towards the contralateral shoulder. This position produces tension across the long thoracic nerve as it passes through the middle scalene muscle. Although direct contact injuries have been reported to cause long thoracic nerve palsy, this mode of injury is relatively uncommon although it is likely underreported. In addition, more generalized neural disorders, such as brachial neuritis, have occasionally been reported to involve the long thoracic nerve [78]. This pain typically occurs along the medial scapular border due to spasm of the unopposed rhomboid musculature. The patient may also complain of mechanical crepitus which can result from scapulothoracic incongruity due to the decreased girth of the atrophied serratus anterior muscle. On physical examination, the patient may be tender to palpation along the medial scapular border. The patient may also exhibit a decrease in active forward elevation of the humerus [114]. There are a few provocative maneuvers that can be performed to detect serratus anterior weakness (discussed further in Chaps. The most useful test, however, is the wall push-up since it has been shown to maximally activate the serratus anterior muscle and to provoke medial scapular winging [115]. To perform the wall push-up, the patient places their hands against a nearby wall at approximately shoulder-height and shoulder-width apart. The patient then performs a push-up as if they were in the prone position while the clinician observes scapular motion.
Purchase viagra soft online. Erectile Dysfunction Treatment: Penile Prosthesis Surgery.