Aditi Borde and Jacqueline Gerhart, Kenan-Flagler Business School, University of North Carolina at Chapel Hill
Contact: Aditi Borde, Aditi_Borde@kenan-flagler.unc.edu
This case study won the 2019 Case Competition sponsored by the Business School Alliance for Health Management (BAHM) and hosted by Harvard Business School’s Health Care Initiative. The competition focused on business-based solutions for incentivizing health behaviors in low-income communities.
Abstract
What is the message?
One-third of Americans are obese1, and obesity is the leading risk factor for developing diabetes2. Rural, low-income diabetics, particularly in North Carolina’s Eastern region, face significant economical and geographical barriers to healthcare. Our proposal leverages a partnership with a retailer like Walmart to bring an incentivized lifestyle management program to diabetics in rural communities. As we continue, we use Walmart as an example, recognizing that there are a number of retailers that we could also partner with. The Convenient Access for Rural Diabetics (CARD) program will provide convenient, one-stop-shopping for key components of diabetes management – healthy foods, exercise, filling prescriptions, regular A1c testing, retinopathy screens, and diabetes education.
The CARD program 1) enrolls diabetics with Blue Cross Blue Shield North Carolina (BCBSNC) insurance and provides them with an activities stamp card. Participants can 2) complete all six Health Initiative Activities at their local Walmart, including buying healthy food in the produce section, filling prescriptions and checking A1c blood levels at booths in the pharmacy, getting retinopathy screenings at the Vision Center, and attending on-site diabetes awareness walks and Walmart Wellness Days both hosted by the American Diabetes Association. For completing each of these Health Initiative Activities, the participants will 3) immediately receive a Walmart gift card as a reward.
What is the evidence?
Analysis by that authors suggests that the projected cost of a relevant program for the first three years is $29.6M. An established company would provide the key infrastructure for the program, and start-up costs will be funded primarily through pharmaceutical company sponsors and grants. The primary revenue stream will come from 50% of BCBSNC’s claims reductions, projected to be $31.7M over three years.
Submitted: January 15, 2019; accepted after review: April 15, 2019.
Cite as: Aditi Borde and Jacqueline Gerhart. 2019. The CARD Program – Influencing Healthy Behaviors in Low-Income Communities. Health Management Policy and Innovation, Volume 4, Issue 1.
Overview
Obesity is associated with lower quality of life and poorer health outcomes, including type II diabetes3-5. Low-income rural diabetics in Eastern North Carolina require healthy diet, exercise, filled prescriptions, regular A1c testing, retinopathy screenings, and health education6-11, yet face significant economical and geographical barriers. A comprehensive diabetes management program is required that 1) aligns with the rural lifestyle, 2) is convenient, 3) brings care into local communities, and 4) supports both financial and physical health. The Convenient Access for Rural Diabetics (CARD) program is unique partnership with Walmart to bring a comprehensive diabetes lifestyle management program into local communities. Participants of the program will earn gift card rewards for buying produce, exercising, filling prescriptions, testing their A1c levels, getting retinopathy screenings, and improving health literacy, all at their local Walmart location.
Background
A person with obesity faces a shorter life with significant health complications, less functional mobility, higher costs with lower pay, and intense social stigma1-5. As a whole, obesity is responsible for driving up US healthcare costs by 29%12. The challenges associated with obesity are not going away, as one in three Americans are currently classified as obese and the rate of obesity has doubled since 198013-14.
Figure 1: Obesity and diagnosed diabetes prevalence by county in North Carolina, 2006-2013
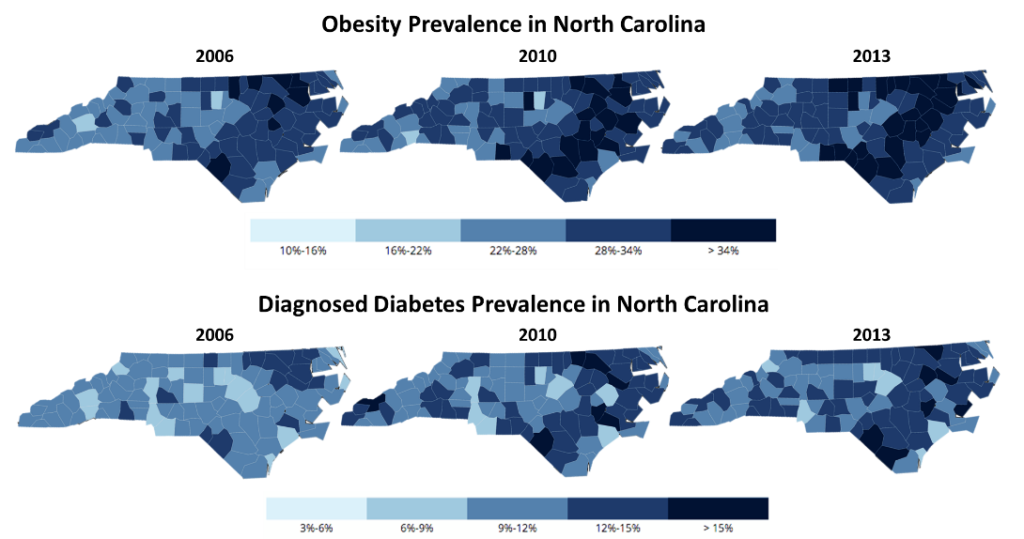
Source: https://www.cdc.gov/diabetes/data/countydata/countydataindicators.html
Obesity is the leading risk factor for developing diabetes2. Studies suggest that approximately 40% of people with obesity experience adverse metabolic events that are precursors to developing diabetes3. Lifestyle-treatment options for diabetes and obesity are very similar, with many studies showing that the critical components for treatment are weight loss and physical activity2,6-7. In the US, 26.1% of people have prediabetes and 9.4% of people have diabetes, with type 2 diabetes accounting for >90% of all diagnosed cases of diabetes in adults15,16.
Target Population and Demographics
North Carolina (NC) has a large population of rural, low-income diabetics who face additional barriers to diabetes care. The rate of the rural population in NC is twice the national rate17, and 93% of counties in NC have diagnosed diabetes rates higher than the national average18. As defined by the NC Association of Local Health Directors, NC is divided into ten regions19. The program will focus on Regions 8, 9, and 10 in Eastern NC because these regions are mostly rural and have the largest diagnosed diabetes percentage by county18. Within the target regions, there are 29 Walmart Supercenters, each with a Vision Center, in-store pharmacy, and groceries (including a produce section)20.
Table 1. Rural versus non-rural Americans
| Rural | Non-rural | |
| Distance to health provider21 | 43.6 miles | 19.3 miles |
| # primary care physicians per 100,000 patients22 | 39.8 | 53.3 |
| Average income22 | $45,482 | $53.657 |
| Uninsured rate23 | 32% | 26% |
| Adults who would describe health status as fair/poor22 | 19.5% | 15.6% |
| Have internet24 | 58% | 80% |
| Have a smartphone24 | 67% | 77% |
Barriers and Solutions
- Cost: In the US, 45% of diabetics have skipped care because of affordability issues, and some patients’ costs have jumped from $300 to almost $1,000 in the last year25.
- The CARD program is free to join, and provides financial incentives to diabetics to manage their disease.
- Low adherence rates: Of type II diabetics, very few are adherent to their prescribed diet regimen (37%), exercise routine (35%), and medications (53%)26.
- The CARD program makes diabetes management convenient, allowing participants to manage their health during their regular shopping.
- Rural geography: Ninety-five percent of NC is a designated Health Professional Shortage Area27, and >25% of Eastern NC people have not seen a doctor in over two years28.
- The CARD program brings comprehensive diabetes management to local communities in a remote healthcare setting, providing one-stop shopping to participants.
- Lack of technology: In the US, 42% of rural residents do not use internet regularly24.
- The CARD program forgoes a digital solution in favor of a back-to-basics solution that all rural residents can use.
- Low health literacy: Nearly 50% of participants in a survey of Southeastern US rural health patients were found to have health literacy difficulties29.
- The CARD program combines the many facets of diabetes care into a single, well-illustrated activities stamp card that is simple to use.
Recommendations
Partnership
Our proposal leverages a unique partnership with Walmart to bring an incentivized lifestyle management program for diabetics to rural, low-income communities. The CARD program encompasses three steps: patient capture, patient activity, and rewards. The program starts when Walmart customers go to the Walmart pharmacy. Upon filling a diabetes prescription, the pharmacy staff member will engage with the patient to tell them about the CARD program and how they can participate. The pharmacist or technician will provide the participant with an activities stamp card and a welcome packet. To maximize enrollment, flyers will be posted at each cash register, encouraging diabetic customers to ask how they can enroll in the CARD program.
Figure 2: Overview of the CARD program
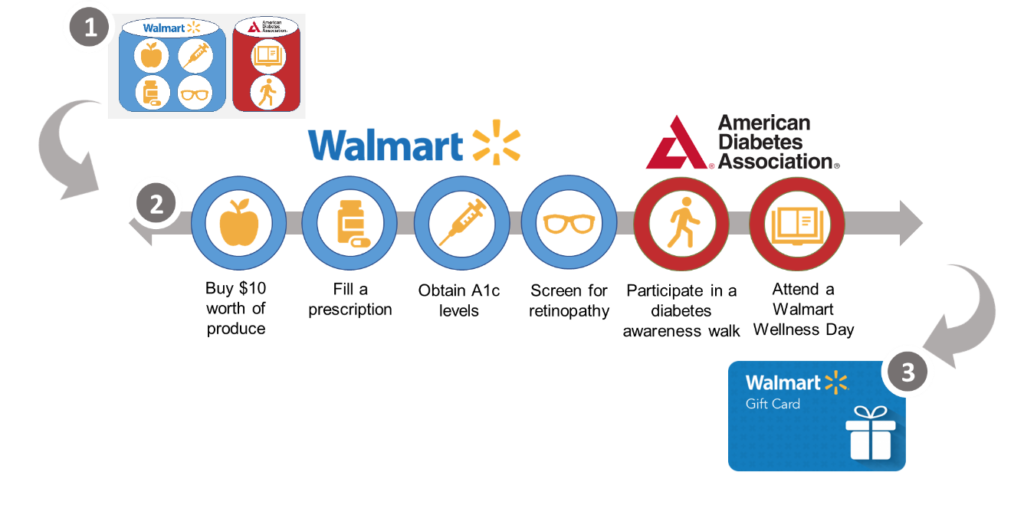
Upon receiving his or her activities stamp card, the participant can partake in the six Health Initiative Activities. When the participant completes one of these activities, he or she will get a stamp on the card and is immediately rewarded with a Walmart gift card redeemable at any brick and mortar location. The number of stamps possible for each of the Health Initiative Activities corresponds to the annual recommended frequency of completing that activity. The amount of the gift card reward for each activity corresponds to the level of participant effort required to complete it, and each participant can earn a maximum of $300 per year.
Table 2. The Six Health Initiative Activities
| Health Initiative Activity | Buy $10 worth of produce | Fill a prescription | Obtain A1c levels | Screen for retinopathy | Participate in a diabetes awareness walk | Attend a Walmart Wellness Day |
| Location | Produce Department | Walmart Pharmacy | Walmart Pharmacy | Vision Center | Parking Lot | Storewide |
| Outcome | Healthy habits | Medication adherence | Regular A1c testing | Preventative health | Exercise | Diabetes education |
| Number of stamps | 12 | 12 | 4 | 1 | 4 | 2 |
| Gift card amount | $5 | $5 | $15 | $20 | $30 | $10 |
The A1c Now+® test will be utilized for point-of-care A1c testing because the test is easy to use, minimally invasive with fast results (less than 5 minutes), FDA-approved and CLIA-waived, and economical (only costs $9 per test)30. A1c-Now+® monitors will be placed in the pharmacy waiting area, where participants can test their blood levels in relative privacy and with pharmacy staff members within reach to offer assistance if needed. There will be space on the back of the activities stamp card for participants to record their A1c level for their reference. These tests will be offered free of charge for all participants. Retinopathy screens will also be free of charge for those who are uninsured or unable to pay.
Walmart currently partners with the American Diabetes Association (ADA) to host quarterly Walmart Wellness Days in which customers can engage with pharmacists to answer health questions and to receive free health screenings. The ADA follows up with interested customers to provide them with physician recommendations. By attending these events, participants can increase their knowledge of how to manage their diabetes, while also increasing clinician engagement. Through the expansion of Walmart’s existing partnership with the ADA, Walmart will host diabetes awareness walks quarterly, which will encourage participants to exercise regularly in a community setting.
Competitive Analysis
The CARD program is currently the only in-person solution that overcomes the rural-urban digital divide to bring diabetes management directly to patients. Omada Health and Virta digital health solutions help patients self-manage their diabetes, providing virtual coaching and diet management support31-32. However, in addition to having a hefty price tag of up to $150/month, these programs also require internet access, which 42% of rural people do not currently have24. Fitness and diet apps are available that link to wearable devices in order to encourage and monitor physical activity, but require internet access and a high degree of health literacy to fully utilize. In-home A1c and glucose monitoring devices, like Dexcom Continuous Glucose Monitoring33, are now available for residential use, but can cost thousands of dollars for patients if they are not covered under insurance. Incentive and online rewards programs are commonly offered through private insurance programs, but again require an internet connection to sign-up and receive rewards. Finally, lifestyle management programs are often offered through healthcare providers. These can be effective in-person solutions, but may require significant travel for those living in rural communities, and can be expensive to the patient.
Table 3. The CARD program versus competitors
| CARD Program | Omada Health31 / Virta32 | Wearables and Lifestyle Apps | Dexcom Continuous Glucose Monitoring33 | Private Insurance Online Rewards Program | Primary Care Provider | |
| Cost | FREE | $130-$400 /month | $100-$300 | $1500 | FREE | $20-$100 per visit |
| Rewards | Favorable | Neutral | Neutral | Neutral | Favorable | Neutral |
| No extensive sign-up | Favorable | Unfavorable | Favorable | Neutral | Neutral | Neutral |
| No technology literacy required | Favorable | Unfavorable | Unfavorable | Unfavorable | Unfavorable | Favorable |
| No internet connection required | Favorable | Unfavorable | Unfavorable | Neutral | Unfavorable | Favorable |
| No smartphone required | Favorable | Unfavorable | Unfavorable | Unfavorable | Favorable | Favorable |
| Does not require travel (convenient) | Favorable | Favorable | Favorable | Favorable | Favorable | Unfavorable |
| Face-to-face interaction | Favorable | Unfavorable | Unfavorable | Unfavorable | Unfavorable | Favorable |
Revenue Model
Over the course of three years, $29.6M will be needed to fund the program. Walmart will provide the primary physical infrastructure for the program. See Supplementary Material for a detailed budget and balance sheet. It is assumed that 25% of participants will adopt the program, and 75% participants will adhere once they begin the program34. Given these assumptions and a 7% growth rate, $8.8M will be required in Year 1, $9.9M in Year 2, and $10.9M in Year 3 ($29.6M in total).
Pharmaceutical companies (e.g. Eli Lilly, Novo Nordisk, Sanofi, and Merck) that manufacture diabetes medications will sponsor the large majority of start-up costs because the CARD program incentivizes diabetics to fill their prescriptions on a regular basis. Additionally, grants from the ADA, NIH National Institute of Diabetes and Digestive and Kidney Diseases, and NC Department of Health and Human Services will fund the remaining upfront costs.
Blue Cross Blue Shield of North Carolina (BCBSNC) will serve as the program’s primary revenue stream. BCBSNC currently holds 96% of North Carolina’s private insurance market share and has significant interest in reducing claims for their members35. If the CARD program decreases BCBSNC’s claims for diabetes-related hospitalizations or related complications by a statistically significant amount, they will pay the program 50% of the cost savings, determined by the difference between actual and expected claims. A participant’s actual year-end claims will be compared to his or her expected claims, calculated from that participant’s average yearly total claims for the past five years. In subsequent years, participants’ expected claims will be extrapolated based on claims from comparable populations (i.e. rural diabetics who are not enrolled in the CARD program).
More than 20% of US healthcare dollars are spent on diabetes36. Diabetes-related hospitalizations and complications can easily exceed $20,000 per patient per hospitalization37. Therefore, even a slight decrease in hospitalizations will have a large impact in decreasing claims paid by BCBSNC. The partnership is low risk, high reward for BCBSNC because if there are not significant cost savings, BCBSNC will not be required pay any money to the program. Reduction in hospitalizations is projected to result in lower rates of cardiovascular disease (5%), ischemic heart disease (6%), stroke (7%), diabetic ketoacidosis (28%), and leg amputations (42%), resulting in a total projected cost reduction of $31.7M over three years.
Implementation
Q2-Q4 2019 will involve contracting with Walmart and BCBSNC, followed by training for managers and customer service, pharmacy, and Vision Center staff on how to administer the program rewards in Q1 2020 – Q2 2020. Q3 2020 – Q4 2020 will involve setting up the infrastructure required to start the program at the 29 Walmart Supercenter locations: distributing welcome packets and activities stamp cards, barcode scanners at the various stations for collecting stamps and rewards, and the A1c-Now blood testing stations in the pharmacies. This will allow for the first site launch in Q1 2021.
Figure 3: Timeline for implementation of the CARD program
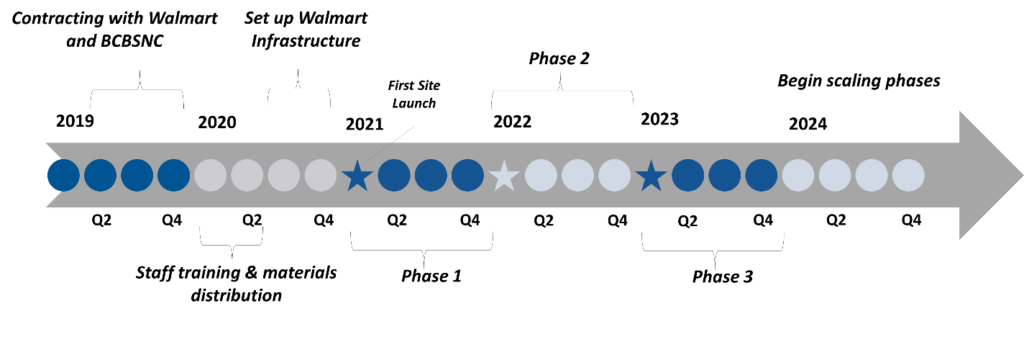
The CARD program will be implemented in phases in order to measure its success at various checkpoints. Phase 1 will involve targeting 5,000 BCBSNC members for enrollment in order to prove the efficacy of the CARD program. In phase 2 of the program, enrollment will be expanded in Q1 2022 by 10,000 members to include both Medicare and Medicaid members and BCBSNC members, as rural low-income patients are more likely than their urban counterparts to have Medicare and Medicaid35. In phase 3, 10,000 additional participants of any insurance type can enroll in the program, bringing total enrollment to ~25,000 participants by Q1 2023.
To conduct performance evaluation of the CARD program, a barcode system will be used to enroll participants in order to link individual participants to their claims data. The activities stamp card will be scanned each time a participant receives a stamp in order to track program adherence. After phase 3 of the program, claims data comparisons of participating and non-participating diabetics will be made annually to determine efficacy of the program, which will transition into quarterly evaluation upon expanded enrollment.
Risk Mitigation
One potential risk with our solution is that Walmart’s participation is necessary to implement the program. However, Walmart stands to gain several key things under our solution. Walmart can expect guaranteed revenue from gift card purchases for program incentives and guaranteed revenue from retinopathy screenings. Gift card use and additional time spent in the store will lead to increased spending by program participants. This solution also aligns with Walmart’s healthcare strategy, since it is seeking to expand into the healthcare space through collaborations with Humana37. With increased use of mail-order prescription services, pharmacies in particular are looking to expand their services. By acting as the point of enrollment and location for A1c testing in the program, pharmacies can achieve this goal. Should Walmart not participate, partnerships with other similar retailers, such as Target, can be pursued.
Another risk is that participants might not modify their behaviors or respond to a rewards program. However, this rewards program is based off of the Transtheoretical Model of Behavior Change38, which was successful in promoting lifestyle changes in a study related to smoking cessation and condom use39. Low-income populations that were provided $10 vouchers for fruits and vegetables yielded voucher redemption rates were approximately 90%40.
Healthcare behavioral modification programs can often face regulatory liabilities. The CARD program is HIPAA compliant, CLIA-exempt, and requires no certificate of need.
Finally, funding could cease for the CARD program. Should this happen, the CARD program is easily modifiable, simple to scale back, and non-labor intensive. Scale backs would not require layoffs and scale ups do not require hiring new employees.
Scaling
The CARD program will be scaled in four phases – by network, geography, partnerships, and disease states. Phase 1 involves expanding beyond payers to providers. Then, extending an invitation to the providers will result in a win-win, because it decreases the cost to the payer while increasing the providers’ connection to the community. Phase 2 involves scaling up across Walmart’s 144 Supercenter locations throughout NC, then scaling to >3500 Supercenters in every part of the United States, allowing for easy market penetration nationwide. In Phase 3, partnerships can be made with other retailers, such as Target, Walgreens, and Costco, to expand the program and enroll more participants. In Phase 4, similar lifestyle management programs can be developed using the CARD program framework that focus on incentivizing patients with other chronic disease states, many of which would entail similar activities (diet, exercise) as diabetes and are also linked to obesity.
Figure 4: Scaling plan for the CARD program

Conclusion
Rural, low-income diabetics, particularly in North Carolina’s Eastern region, face significant economical and geographical barriers to healthcare. We are proposing a partnership with Walmart to bring an incentivized lifestyle management program to diabetics in rural communities. The Convenient Access for Rural Diabetics (CARD) program will provide convenient, one-stop shopping for key components of diabetes management. The CARD program 1) enrolls diabetics and provides them with an activities stamp card. Participants can 2) complete all six Health Initiative Activities at their local Walmart, including buying healthy food in the produce section, filling prescriptions and checking A1c blood levels at booths in the pharmacy, completing a health risk assessment at the Pursuant Health kiosk, and attending on-site diabetes awareness walks and Walmart Wellness Days, both hosted by the American Diabetes Association. For completing each of these Health Initiative Activities, the participants will 3) immediately receive a Walmart gift card as a reward. Reductions in hospitalizations as a result of our proposal are predicted to result in more than $30M in cost savings in the first three years of implementation, with many potential ways to scale the CARD program to reach as many diabetics as possible.
- https://www.nhlbi.nih.gov/health/educational/wecan/healthy-weight-basics/obesity.htm
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066828/
- https://www.jci.org/articles/view/78425
- https://news.harvard.edu/gazette/story/2012/03/the-big-setup/
- https://www.sciencedirect.com/science/article/abs/pii/S1521690X13000365
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5426415/
- http://care.diabetesjournals.org/content/39/11/2065
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4966497/
- https://www.ncbi.nlm.nih.gov/pubmed/29740786
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5800256/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1424643/
- https://www.sciencedaily.com/releases/2018/02/180208180356.htm
- https://www.cdc.gov/obesity/data/adult.html
- https://www.hsph.harvard.edu/news/press-releases/worldwide-obesity/
- https://www.cdc.gov/diabetes/basics/type2.html
- https://www.cdc.gov/media/releases/2017/p0718-diabetes-report.html
- https://www.northcarolinahealthnews.org/2018/01/22/n-c-rural-health-numbers/
- https://www.cdc.gov/diabetes/data/countydata/countydataindicators.html
- http://www.ncalhd.org/map/
- https://www.walmart.com/store/finder
- https://www.shsu.edu/centers/rural-studies/TRS/TRS%202013%20Health%20Report.pdf
- https://www.ruralhealthweb.org/about-nrha/about-rural-health-care
- https://www.ncchild.org/whats-right-solution-health-care-rural-north-carolina/
- http://www.pewresearch.org/fact-tank/2017/05/19/digital-gap-between-rural-and-nonrural-america-persists/
- https://www.usnews.com/news/health-care-news/articles/2018-06-18/study-almost-half-of-diabetics-skip-care-because-of-high-cost
- http://clinical.diabetesjournals.org/content/24/2/71
- https://files.nc.gov/ncdhhs/documents/2018%20HPSA%20Full%20Map.jpg
- https://schs.dph.ncdhhs.gov/data/brfss/2015/nc/nccr/topics.htm#ds
- https://rnojournal.binghamton.edu/index.php/RNO/article/download/187/162/0
- https://ptsdiagnostics.com/a1cnow-plus-system/
- https://go.omadahealth.com/
- https://www.virtahealth.com/
- https://www.dexcom.com/
- https://www.ncbi.nlm.nih.gov/pubmed/17044763
- https://www.kff.org/state-category/health-coverage
- https://asmbs.org/resources/weight-and-type-2-diabetes-after-bariatric-surgery-fact-sheet
- https://www.wsj.com/articles/walmart-in-early-stage-acquisition-talks-with-humana-1522365618
- http://sphweb.bumc.bu.edu/otlt/MPH-Modules/SB/BehavioralChangeTheories/BehavioralChangeTheories6.html
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5486267/
- https://www.sciencedirect.com/science/article/pii/S0002822306001416
{kind=link}